Investigating inequalities in cancer incidence, mortality and DALY rates among women worldwide is extremely important. This issue is not only relevant to women’s health and quality of life but also impacts the social and economic development of societies [7]. Various factors, including biological, social, and cultural influences, may put women at higher risk for developing certain types of cancer [7]. Inequities in access to healthcare, education, and cancer awareness—particularly in low- and middle-income countries can result in late diagnoses and poor treatment. This impacts women’s health and burdens families and healthcare systems [9]. Therefore, gaining a comprehensive understanding of these inequalities is crucial for designing effective policies and programs that promote women’s health and reduce the incidence of cancer.
BC is the most common cancer diagnosed in 2020, with 2 million new cases. The incidence and mortality rates of this disease have increased over the past 3 decades [10]. The availability of mammography as a reliable screening tool [11], along with policies aimed at reducing the burden of BC in many countries [12] and increased awareness among women about the disease [13], has contributed to a rise in the incidence of this malignant tumor globally. However, the high rate of BC in countries with a high HDI can be attributed to several factors. These include a greater prevalence of risk factors associated with BC (early age at menopause, advanced age at first birth, limited breastfeeding, use of menopausal hormone replacement therapy and oral contraceptives, higher body mass index, lack of physical activity) in these societies, as well as the availability of well-established screening programs [14, 15].
The results of this study indicated that there is no inequality in BC mortality rates among different countries. One possible reason for this finding could be deficiencies in data collection in countries with low HDI, which may lead to the undercounting and underreporting of BC death rates [16]. Also, international initiatives aimed at improving BC care in countries with low HDI may have resulted in better outcomes for patients. Programs funded by global health organizations can enhance the detection, treatment, and education surrounding BC [17]. In conclusion, although one might expect to see disparities in BC mortality rates based on HDI, these international initiatives and support have helped create a more equitable situation. In addition, in high HDI countries, disparities in healthcare access due to socioeconomic status, race, and ethnicity contribute to higher mortality rates among low-income and marginalized groups, despite effective treatments. In low HDI countries, economic constraints further limit access to treatments, which results in higher BC mortality rates among impoverished communities in wealthy and poorer countries, highlighting a common issue.
DALYs represent the total years of healthy life lost due to illness and disability, and the burden of cancer mortality in terms of years of life lost [18]. Generally, individuals in countries with a higher HDI tend to live more years with disability, while those in countries with a lower HDI experience a greater burden of premature mortality. As a result, although countries with higher HDI have a greater share of the BC incidence burden, the DALY for BC is relatively similar in both high and low HDI countries [19].
OC ranks as the eighth most common cancer globally, accounting for 3.7% of all cancer cases and 4.7% of cancer-related deaths among women in 2020. In developed countries, it is the sixth most prevalent cancer and the fifth leading cause of cancer death among women [20, 21]. Before the year 2000, the age-standardized incidence of OC was highest in North America and Northern Europe; however, these rates have since declined in these regions while increasing in Asia and Eastern Europe [21].
UC is the fourth most common cancer among females and the sixth leading cause of cancer-related deaths in the U.S. In 2023, an estimated 66,200 new cases and 13,030 deaths are expected. Its incidence is rising and is projected to surpass colorectal cancer by 2040, becoming the third leading cancer among females and the fourth leading cause of cancer death [22]. In 2021, the age-standardized incidence rate (ASIR), age-standardized prevalence rate (ASPR), age-standardized mortality rate (ASMR), and age-standardized DALY rate (ASDR) of UC in China were 6.65, 46.52, 1.24, and 37.86 per 100,000 population, respectively [23]. In the UK, UC is the fourth most common cancer among females, with approximately 9,800 new cases diagnosed each year. This type of cancer accounts for 5% of all new cancer cases in females in this country, the incidence rates of UC are highest in women aged 75 to 79 [24].
UC has three main histologic types: endometrioid, non-endometrioid, and sarcoma. Endometrioid cancers, comprising about 75% of cases, have the best prognosis. Non-endometrioid cancers, including serous and clear cell carcinomas, account for 15–20% and are more aggressive with poorer outcomes. Uterine sarcomas, arising in the myometrium, are the rarest and least studied [22]. The results of this ecological study indicated that increasing HDI and its components caused the incidence, mortality, and DALY rates of OC and UC to increase.
Early detection and screening for OC and UC are challenging because the disease often lacks specific symptoms. While there is a global shortage of reliable screening methods, countries with high HDI have an advantage due to better healthcare systems and greater access to modern imaging techniques. Consequently, the incidence rate of OC and UC are higher in these countries [25]. In contrast, in low HDI countries, it is not uncommon to fail to diagnose OC and UC until it has metastasized or misdiagnose it for a different type of cancer or even a different disease [25]. In high HDI countries, some risk factors such as overweight, obesity, smoking, and nulliparity occur more frequently than in low HDI countries, leading to a higher incidence of OC and UC [26, 27].
One of the causes of inequality in OC and UC mortality rates could be late diagnosis and lack of access to adequate treatment, including complex surgeries and chemotherapy regimens, particularly in countries with low HDI [28]. However, our study found that the OC and UC mortality rate in high HDI countries is higher than in low HDI countries because the absolute number of deaths is largely proportional to the incidence of the disease, therefore, developed countries tend to demonstrate improved mortality/incidence ratios due to advancements in detection and treatment. In general, low HDI have intermediate to low absolute mortality rates, but high mortality/incidence ratios in OC and UC [25]. In countries with a high HDI, patients with OC, UC tend to live longer because they have better access to timely diagnostic services and more effective treatment options [29]. As a result, these countries have a DALY Index compared to countries with a low HDI.
In addition, in high-HDI countries, molecular diagnostics for classifying and stratifying treatment for endometrial cancer are becoming increasingly common [30]. Tumor molecular classification in early-stage, high-risk endometrial cancer has proven to be cost-effective [31]. As a result, the prevalence rate of UC is higher in these countries. Consequently, because tumor molecular classification influences the choice of treatment, the DALY rate of UC is also higher in high-HDI countries compared to those with low HDI. However, their high costs may exacerbate inequalities if not equitably accessible.
CC is the second most common malignant tumor among females worldwide and poses a significant threat to women’s health. Persistent infection with high-risk Human Papillomavirus (HPV) has been identified as the primary cause of CC, the clear etiology accelerated the establishment and implementation of comprehensive prevention and control system of CC [32]. In 2018, there were an estimated 570,000 cases of CC globally, resulting in 311,000 deaths. Globally, the incidence of CC cases increased from 335,641.56 in 1990 to 565,540.89 in 2019 [33].This makes CC the fourth most commonly diagnosed cancer and the fourth leading cause of cancer-related deaths in women.
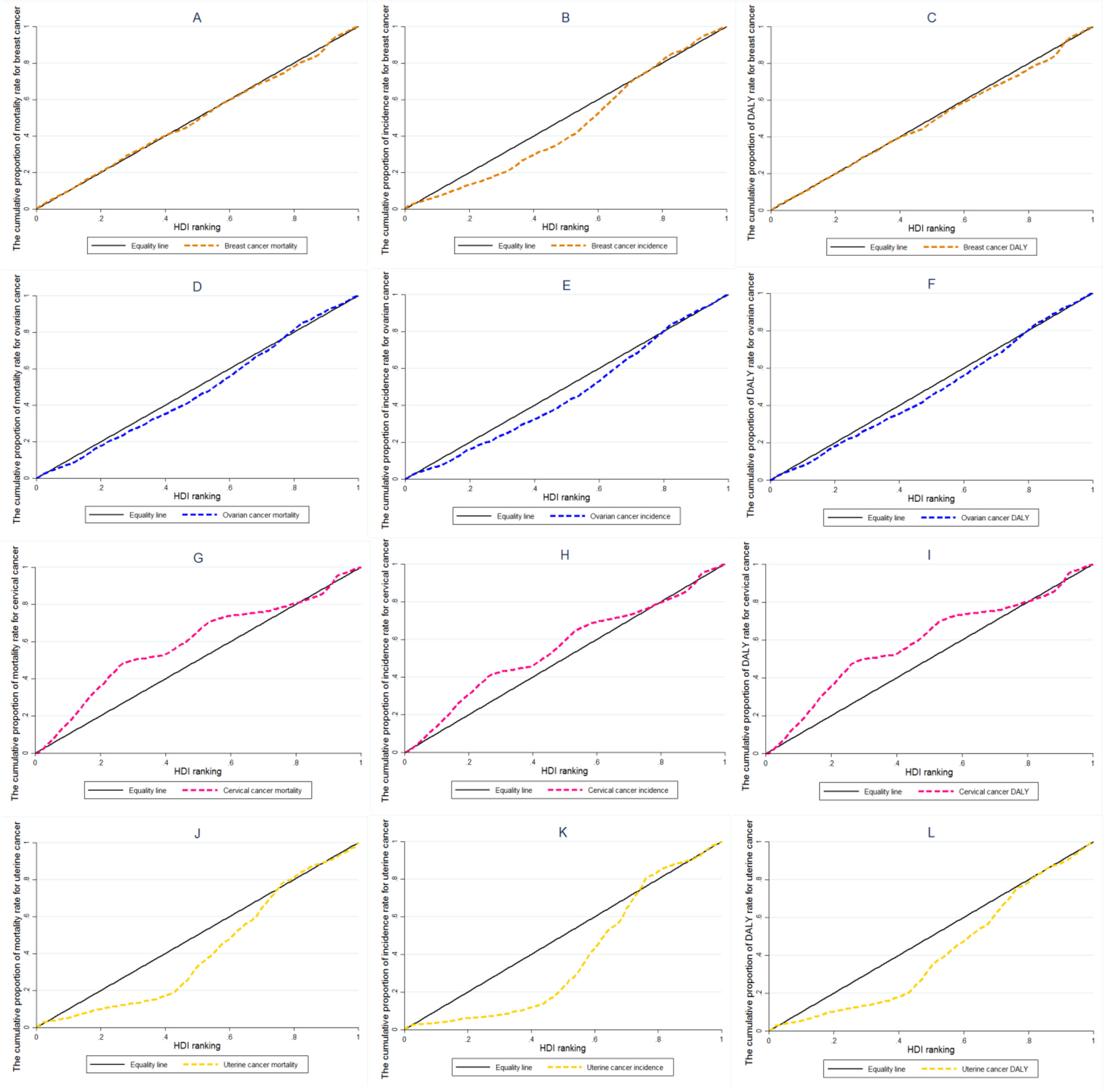
Notably, approximately 85% of CC deaths occur in underdeveloped or developing countries [34]. The death rate from CC is 18 times higher in low-income and middle-income countries compared to wealthier nations [35]. Consistent with the above, our ecological study showed that the incidence and mortality rates of CC are higher in countries with low HDI. The 20% of the world’s population with the lowest HDI had an incidence and mortality rate for CC that accounted for approximately 35% of global cases. In contrast, the same percentage of the population with the highest HDI represented only about 0% of CC cases.
On November 17, 2020, the WHO released a global strategy aimed at accelerating the elimination of CC as a public health problem. This marked a historic commitment, with 194 countries pledging to work together to eradicate CC for the first time. According to the WHO strategy, countries must maintain an incidence rate below 4 cases per 100,000 women by achieving the 90–70–90 targets by 2030. These targets include: 90% of girls fully vaccinated with the HPV vaccine by age 15, 70% of women screened using a high-performance test by the ages of 35 and 45, and 90% of women with pre-cancerous conditions and invasive cancer receiving treatment [36], However, only 78 countries reported on HPV immunization programs, with 85% of them being high HDI countries [37].
The low incidence of CC in countries with high HDI is due to the inclusion of HPV vaccination in the general vaccination program, which has subsequently led to a decrease in positive cases of high-risk HPV strains and a decrease in positive Pap test [38]. Following the decline in incidence, mortality, and DALY rates have also decreased in these countries. Although screening rates for CC are lower in low HDI countries compared to high HDI countries, the limited coverage of HPV vaccination in low HDI countries results in a higher number of positive PAP test results, which contributes to an increased incidence of CC [38]. Furthermore, low health literacy among women in these regions often leads to delayed referrals and diagnoses at more advanced stages of the disease. Additionally, limited access to healthcare services in low- and middle-income countries contributes to higher mortality rates from CC [37]. Implementing widespread HPV immunization could help address this inequity [37].
The standard surgical treatment for CC at stage IA2-IIA involves radical hysterectomy combined with pelvic lymphadenectomy, with or without adjuvant chemo-radiation [39]. This treatment results in the loss of fertility for women of reproductive age and an increased DALY. However, with the development of minimally invasive surgical techniques such as vaginal trachelectomy and robotic-assisted radical trachelectomy, fertility can be preserved and DALY rates can be reduced in these patients [40].
At last, we suspect that the COVID-19 pandemic may have affected our study results. In general, this pandemic has a significant impact on cancer incidence and mortality, including breast, cervical, ovarian and uterine cancers. Travel restrictions and concerns about the spread of the virus have led to a decrease in regular check-ups and cancer screenings, which can lead to late diagnosis and an increase in the incidence of these diseases. In addition, health services have been strained and many patients have delayed treatment, with a direct impact on mortality and disability-adjusted life years (DALYs). Preliminary estimates suggest that these changes are being felt particularly by vulnerable groups, who typically have less access to health services, and may lead to an increased burden of disease in the future [41].
Our study had some limitations. First, since this is an ecological study, the exposure data is presented at an aggregate level. This requires us to exercise caution when interpreting the results to avoid ecological fallacy. Ecological fallacy occurs when a relationship observed at a group level does not accurately represent the association at an individual level. Another limitation of ecological studies is the difficulty in controlling for confounding variables. In addition, data gaps in cancer registries, particularly in low-HDI countries, may bias RCI estimations. This is especially true for cancers with a high risk of underreporting, such as cervical and uterine cancer. Due to these limitations, ecological studies are less effective for conclusively testing causal hypotheses. However, they can be useful for generating hypotheses for further investigation.