As one of the most commonly employed surgical procedures, total knee arthroplasty (TKA) has been widely used for treating knee joint disorders and degenerative arthritis. Despite the substantial clinical value and advancements in the surgical technique itself, postoperative complications remain a critical factor affecting patients’ quality of life and physical and psychological well-being [13]. At present, the prediction and prevention of postoperative complications constitute key areas in clinical research. However, the predictive utility of biomarkers such as fat infiltration, muscle parameters, and hematologic indicators remains inconclusive. Therefore, the present study aimed to investigate the potential of novel fat infiltration, muscle parameters, and hematologic indicators in predicting severe postoperative complications following TKA. Identifying potential risk factors preoperatively could provide more detailed references for clinical decision-making, thereby improving prognosis and reducing the incidence of complications.
In this study, postoperative complications were observed in 32 out of 168 TKA patients, accounting for 19.05%, indicating that severe complications are relatively common after TKA and should be given heightened clinical attention. Previous research has shown that extensor mechanism injuries—such as patellar tendon rupture, quadriceps tendon rupture, or tibial tubercle avulsion—are frequent complications following TKA and can lead to joint dysfunction, sometimes requiring revision surgery [14]. Additional findings have demonstrated a positive correlation between the ratio of fat to muscle area measured via MRI and postoperative complications, whereas no significant correlation has been found with BMI, suggesting that muscle parameters may more accurately reflect the risk of complications than BMI, thereby supporting the results of the present study [15]. Fat infiltration is defined as the presence of adipocytes within the interstitium of tissues and organs that normally lack fat cells. It serves as an indicator of body fat distribution and muscle health. Appendicular skeletal muscle mass effectively reflects the quality and quantity of limb musculature, with reduced muscle quality constituting a novel marker of fat infiltration. It has been established that skeletal muscle quality is closely associated with joint stability and function. In TKA patients, poor skeletal muscle quality is often related to impaired knee function, delayed postoperative recovery, and increased pain. Insufficient muscle mass may also indicate a lack of strength necessary for rehabilitation support. A decrease in muscle mass is usually accompanied by a higher proportion of fat, and poor muscle quality may impair immune function, thereby increasing the risk of postoperative infections [16]. Furthermore, inadequate muscle quality has been shown to adversely affect blood circulation, elevating the risk of venous thromboembolism. This is particularly relevant during the early postoperative period, when patients remain bedridden for extended durations. In such cases, the lack of muscle activity may slow blood flow and promote thrombus formation [17].
It has been reported that fat infiltration directly affects muscle structure, diminishing muscle strength and functionality, especially during postoperative rehabilitation in TKA patients. Patients with poor preoperative muscle quality may experience delayed recovery. Fat infiltration also impairs muscle function, destabilizing the knee joint, and may lead to gait abnormalities and muscle atrophy. Variations in muscle quality after surgery directly affect knee function and recovery. Patients with greater fat infiltration typically face longer rehabilitation periods and a higher risk of postoperative complications [18]. Recent studies have identified waist circumference (WC) as a proxy for central obesity or overall adiposity. It has been shown to be a more accurate predictor of cardiometabolic morbidity and mortality than BMI, as BMI does not account for fat distribution. Central obesity measured by WC has been strongly linked to severe complications following TKA, and WC-based screening and intervention strategies may assist orthopedic surgeons in risk stratification for patients with elevated BMI [19]. As a critical index for assessing body fat distribution, WC plays a vital role in predicting complications after TKA. Postoperatively, many patients experience restricted mobility, predisposing them to circulatory disturbances. Individuals with higher WC values often possess substantial abdominal adipose tissue, which can hinder venous return and elevate the risk of deep vein thrombosis (DVT). Abdominal fat may exert compressive effects on venous flow, further exacerbating thrombogenesis [20].
The incidence of postoperative complications in TKA patients is commonly influenced by multiple factors. Among these, muscle density has emerged as a novel predictive indicator and has garnered increasing academic attention. Muscle density refers to the concentration of muscle tissue per unit volume and is closely associated with muscle quality and strength. Studies have indicated [21] that muscle density may be strongly related to the rate of postoperative recovery, the occurrence of complications, and overall rehabilitation outcomes.
In the present study, muscle density was found to be an effective predictor of severe postoperative complications in TKA patients and was identified as an independent risk factor. Previous research has demonstrated [22] that patients with reduced muscle density are at significantly higher risk of complications after TKA, including infection, prosthesis loosening, and prolonged hospitalization, thereby further corroborating our findings. Muscle density serves as an indicator of muscle health and strength reserve. Higher muscle density reflects greater muscle strength and better functional capability, whereas lower density is often accompanied by muscle atrophy, metabolic disorders, and muscular insufficiency. The rehabilitation process following TKA generally depends on the patient’s muscle recovery status, and changes in muscle strength and density directly influence knee joint stability and functional recovery. Patients with lower muscle density often exhibit compromised immune function, making them more susceptible to postoperative infections. Furthermore, muscle not only supports joint stability but also plays a direct role in modulating immune responses [23]. Inadequate muscle density can compromise knee joint stability, limit functional recovery, and increase the risk of revision surgery. Weaker musculature may also fail to provide adequate joint support, thereby impeding postoperative recovery. Consequently, muscle density may serve as a valuable predictive marker to help clinicians evaluate postoperative recovery and complication risk.
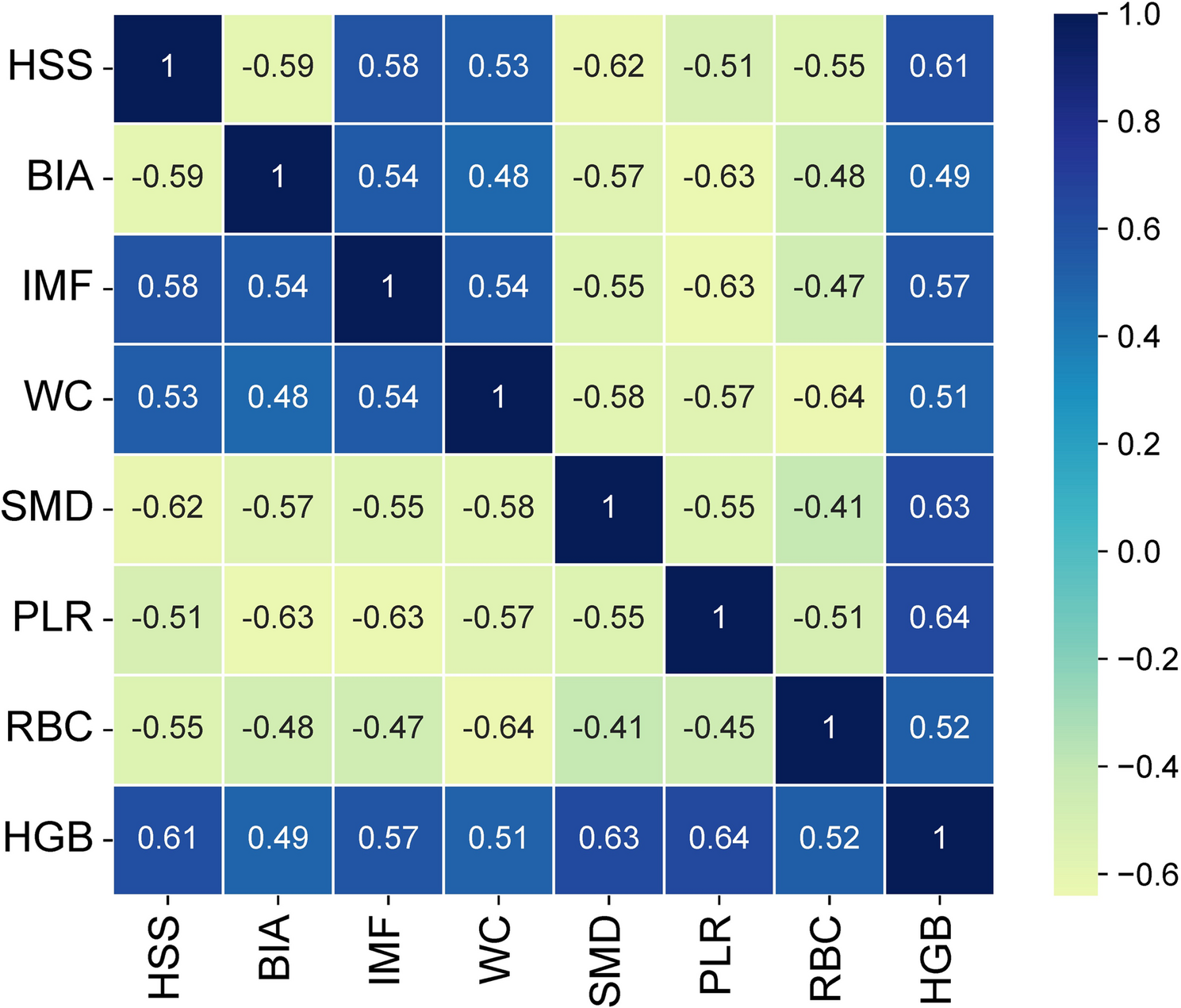
In recent years, hematologic indicators have gained attention as tools for predicting postoperative complications, including PLR, red blood cell count, and hemoglobin (HGB), which may have potential associations with adverse outcomes. The present study found that these hematologic parameters (PLR, RBC count, and HGB) were effective in predicting severe postoperative complications in TKA patients. It has been shown [24] that elevated PLR is associated with a higher likelihood of postoperative infection, as an increased PLR reflects a stronger inflammatory response. Inflammation facilitates bacterial invasion by provoking excessive immune responses at the surgical site, particularly in patients with weakened immune systems, who are at greater risk of infection [25]. Recent evidence suggests [26] that patients with lower postoperative red blood cell counts are more vulnerable to infections due to impaired immune function. A decline in RBC count may also compromise oxygen delivery, thereby impairing wound healing and elevating infection risk. Furthermore, it has been found [27] that lower HGB levels may signal weakened immune function and reduced oxygen transport, which negatively affects the functionality of immune cells and wound healing capacity, thereby increasing susceptibility to infection—especially in anemic patients, who are at significantly higher risk of postoperative infections. Additional research [28]has indicated that HGB levels are closely associated with blood viscosity and coagulation function. Variations in HGB may lead to increased blood viscosity or coagulation abnormalities, which in turn directly elevate the risk of thrombosis [29]. In the multivariate analysis, the P-values for muscle fat infiltration and WC were greater than 0.05, possibly due to a weaker association with postoperative complications after TKA or the influence of other factors such as sample size, confounding variables, or interference from other predictors. The clinical relevance of these findings requires further investigation, and more complex statistical models accounting for interaction effects should be considered.
Limb skeletal muscle content is significantly correlated with postoperative functional recovery, and low skeletal muscle content may increase the risk of postoperative infection and prosthetic loosening [30]. Patients with lower skeletal muscle mass have longer recovery times and higher complication rates. Muscle fat content and the degree of fatty infiltration are closely related to postoperative infection and poor functional recovery, with obese patients having a significantly higher risk of complications. While WC is associated with the risk of deep vein thrombosis (DVT), its direct predictive value is limited and is more often used as a surrogate marker for obesity. Muscle density reflects muscle quality, and low density is associated with poor postoperative functional recovery and an increased risk of periprosthetic fractures. PLR, as an inflammatory marker, suggests that a high PLR may indicate an increased risk of postoperative infection. Low red blood cell count or HCT is associated with postoperative anemia and may increase the need for transfusions and infection risk. Moreover, indicators such as limb skeletal muscle content, muscle fat content, WC, muscle density, PLR, red blood cell count, and HCT have important clinical significance in predicting postoperative complications following total knee arthroplasty (TKA). These indicators may serve as independent risk factors in prediction models, improving the accuracy and clinical application value of predictions. Future research should further explore the use of these indicators in predictive models and optimize the construction and validation of these models [31]. In addition, muscle-related parameters (fat content, density, skeletal muscle mass) demonstrate clear mechanisms and outstanding efficacy in predicting TKA complications, while traditional indicators (WC, HCT) are more suitable for rapid screening. Clinically, a “muscle phenotype-driven, inflammation/metabolic marker-assisted” stepwise predictive system should be established, while promoting the standardization, dynamization, and intelligent development of muscle assessment technologies.
Nevertheless, several limitations exist in this study. The sample size was relatively small, and the cohort was demographically homogeneous, which may limit the generalizability of the findings. Although the study controlled for some confounding variables through clinical data comparison, it was unable to completely eliminate the influence of all confounding factors. For instance, unmentioned confounders in the study (such as surgical technique, postoperative care, and patient compliance) may have impacted the results. Additionally, as this is a retrospective study, it has inherent limitations, such as recall bias and selection bias. Moreover, retrospective studies face limitations in conducting strict randomized controlled trials through prospective design, so there are constraints in inferring causal relationships. The study did not mention validation through prospective research or animal models (such as mouse experiments) to further confirm the generalizability and mechanisms of the conclusions. Future studies should consider incorporating multicenter, multi-ethnic, and diverse diabetes types in the patient population to enhance the representativeness of the research. The study also did not clearly mention fully adjusting for all known confounding factors that might affect the results (such as diabetes, antibiotic use, surgical time, postoperative care, etc.), which could affect the accuracy of the results. Due to the lack of prospective research and animal model validation, there are limitations in drawing causal inferences, making it difficult to determine the direct causal relationships between specific factors (such as obesity, diabetes, etc.) and postoperative complications.
Although the study found that severe complications after TKA are related to multiple factors, such as preoperative nutritional status, surgical technique, surgery type, surgical time, and postoperative care, the specific mechanisms have not been fully elucidated. This study is retrospective, and while clinical data comparison was used to control for confounding variables, not all confounders could be eliminated. To address this, future clinical research should expand sample sizes and include multicenter, multi-ethnic, and diverse diabetes types to validate the generalizability of the conclusions. Additionally, in vivo animal models (such as mouse experiments) should be conducted for validation, and multivariable analysis or matching designs should be used to reduce interference.
Confounding factors are variables that are related to both the exposure and the outcome, and their presence may lead to bias in the research results. For example, preoperative activity levels may be related to postoperative complications but were not included in the analysis, which could lead to bias in interpreting the results. To control for potential confounders during the research design phase, various methods can be employed, such as randomization, restriction, matching, and stratified analysis, which can reduce the impact of confounders. Additionally, during the analysis phase, statistical methods (such as regression analysis, stratified analysis, and propensity score matching) can be used to adjust for the influence of confounders.
In conclusion, postoperative complications are common among TKA patients and may be influenced by factors such as appendicular skeletal muscle mass, muscle fat infiltration, waist circumference, muscle density, PLR, red blood cell count, and hematocrit. These parameters may serve as important clinical tools for evaluating patient prognosis and provide a scientific foundation for personalized treatment strategies.