This case represents the report of D. micraerophilus-associated bacteremia originating from a submandibular gland abscess, differing from prior reports limited to genitourinary sources. The underlying SS likely constituted a predisposing factor. SS is characterized by lymphocytic infiltration and glandular destruction of the salivary and lacrimal glands, resulting in decreased salivary gland function [10, 11]. This dysfunction alters oral microbiota diversity, typically manifesting as reduced microbial richness compared to non-SS individuals [12]. Moreover, the relative abundance of Dialister spp. is significantly increased in patients with SS, often rendering it a dominant component of the oral microbiota [13, 14].
In the present case, D. micraerophilus infection led to submandibular gland abscess formation. The underlying mechanism may involve its high oral abundance, which activates macrophages and neutrophils, inducing local inflammation through a process similar to the lipopolysaccharide-mediated inflammatory response caused by Porphyromonas gingivalis [7]. Persistent inflammation contributes to ductal obstruction and secretion retention, facilitating abscess formation. Increased vascular permeability within the abscess wall then permits bacterial translocation into the bloodstream, resulting in bacteremia.
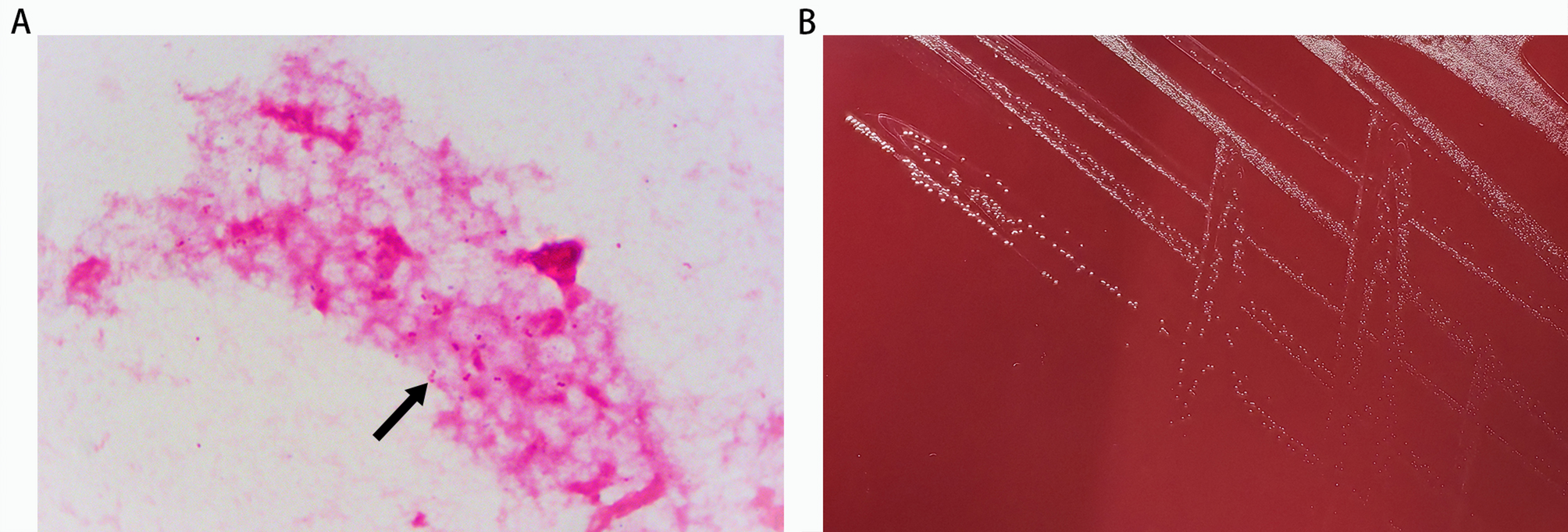
D. micraerophilus is a slow-growing anaerobic or microaerophilic bacterium that is challenging to isolate and propagate from primary cultures [9]. In this case, the organism was detected in blood cultures but not in aspirated pus. This discrepancy may have been due to prior empirical treatment with piperacillin-tazobactam, to which the organism was susceptible, as confirmed by antimicrobial susceptibility testing. This likely inhibited bacterial growth in the abscess specimen, leading to culture failure. However, D. micraerophilus was subsequently confirmed through mNGS of the abscess fluid, further validating its role in the infection.
The patient was initially treated with intravenous piperacillin-tazobactam 4.5 g every 8 h, in line with first-line therapy for submandibular gland abscess as recommended by “The Sanford Guide to Antimicrobial Therapy” [15]. During treatment, a bloodstream infection was confirmed. Serial monitoring demonstrated significant reduction in inflammatory markers and abscess resolution, supporting the completion of a 10-day course. Following confirmation of susceptibility to amoxicillin-clavulanate, oral therapy with amoxicillin-clavulanate 0.375 g every 8 h was prescribed post-discharge, achieving clinical cure after a total of 3 weeks of antimicrobial therapy. Previously reported D. micraerophilus infections resolved with similar regimens: one pyometra case managed with sequential cefmetazole followed by amoxicillin-clavulanate, and one Bartholin’s gland abscess treated entirely with amoxicillin-clavulanate [1, 9]. These outcomes corroborate the efficacy of amoxicillin-clavulanate against D. micraerophilus.
This study still has certain deficiencies. First, the lack of DNA isolation and 16 S rRNA sequencing analysis of salivary samples from both active-infection and recovery phases precludes validation of the hypothesis that oral microbiome enrichment of Dialister spp. contributed to this infection. Second, the therapeutic approach complicates clinical interpretation: initial intravenous piperacillin-tazobactam was followed by sequential oral amoxicillin-clavulanate upon discharge. This regimen obscures definitive assessment of amoxicillin-clavulanate monotherapy efficacy against D. micraerophilus-associated bacteremia due to confounding by prior therapy.
In conclusion, this case describes SS complicated by a submandibular gland abscess with concomitant bacteremia due to D. micraerophilus. Sequential treatment with piperacillin-tazobactam followed by amoxicillin-clavulanate achieved full clinical resolution. Clinical recommendations include providing oral hygiene education to patients with SS and emphasizing the importance of strict aseptic techniques by dental practitioners during invasive procedures to reduce infection risks.