Hantavirus infection is emerging as a global health concern, but the exact prevalence of the disease in Sri Lanka remains unclear. This study aimed to identify early-stage and mild/atypical forms of hantavirus infection among clinically suspected dengue patients who tested negative for dengue. Among the tested patients, 79.5% tested negative for dengue, highlighting the potential for misdiagnoses and delays in accurate diagnosis. These challenges are common in patients presenting with dengue-like symptoms, emphasizing the importance of prompt and accurate diagnoses. Early identification is crucial for effective patient management, epidemiological analysis, and the development of preventive strategies and future research.
Prevalence and demographic profile of probable hantavirus infections
The study found a 5.1% positivity rate for hantavirus among clinically suspected dengue patients, which is consistent with similar studies in the region [18, 19]. For instance, a study in Indonesia reported a 4.23% prevalence of hantavirus among dengue-like patients, while a Cambodia study showed a 4% prevalence [20, 21].
In-house real-time RT-PCR assay used for detection of hantavirus RNA was replication of method originally described by Mohamed et al., in 2013. It is SYBER green based real-time RT-PCR which has ability to detect L segment of the hantavirus genome which is the most conserved part of the viral genome in different type of hantavirus clade with analytical sensitive of less than 100 RNA copies/mL (15). Assay was validated locally by using synthetic genes of 12 different types of hantaviruses kindly provided by the authors described this assay originally. The commercial immunoblot assay (Mikrogen recomLine HantaPlus IgM, Mikrogen, Germany) has sensitivity of 98.3% and specificity of 94.1%, based on product broacher. There is no recorded cross reactivity with other virus or bacterial antibodies except antibodies against Sand fly fever virus (SSFV) and anti-malaria antibodies. Assay itself has test line for SSFV. And there was no evidence of other Bunyavirus infections in the country other than hantaviruses and malaria was eliminated since 2016. This test assay was used in previously published serological studies on hantaviruses in Europe [22, 23].
Interestingly, none of the study samples tested positive for hantavirus RNA, which could be due to factors such as low-level viremia or a short duration of viremia [24]. Hantavirus infection may present with a transient or low viral load, which may not be detectable during the sampling period [25]. In addition to that timing of sample collection and suboptimal sample handling before sending in to laboratory may have contributed for negative PCR results. Instead, Hantavirus IgM antibodies, which can remain detectable for 3–4 months after infection, may indicate recent past exposure to the virus [26]. Demonstration of four-fold rise of hantavirus IgG is confirmatory; however, it was not performed due to logistical reasons. Despite the presence of hantavirus IgM antibodies, these patients tested negative for other common febrile illnesses, including dengue, alphavirus infections, and leptospirosis, helping to narrow the potential causes of their symptoms. Therefore, these cases can be considered as probable or suspected hantavirus cases. All hantavirus IgM positive samples gave positive band on Hantaan virus nucleocapsid antigen coated region and majority has given bands on Hantaan, Dobrava and Seoul virus antigens coated region indicating infection could be due to hantavirus which antigenically related to Hantaan, Dobrava and Soul viruses. Serological evidence of Hantaan virus or Hantaan-like virus has detected in Sri Lanka previously and serological cross reactivity was noted [10, 14].
Additionally, six samples tested positive for flavivirus PCR, which confirmed these cases as dengue infections. Initially, these cases were negative for the NS1 antigen but were later confirmed as dengue through PCR. This discrepancy may be attributed to the low sensitivity of NS1 detection, particularly in secondary dengue cases, where the immune response might not produce detectable levels of the NS1 antigen [27]. This highlights the need for multiple diagnostic methods to accurately identify and differentiate between similar febrile illnesses.
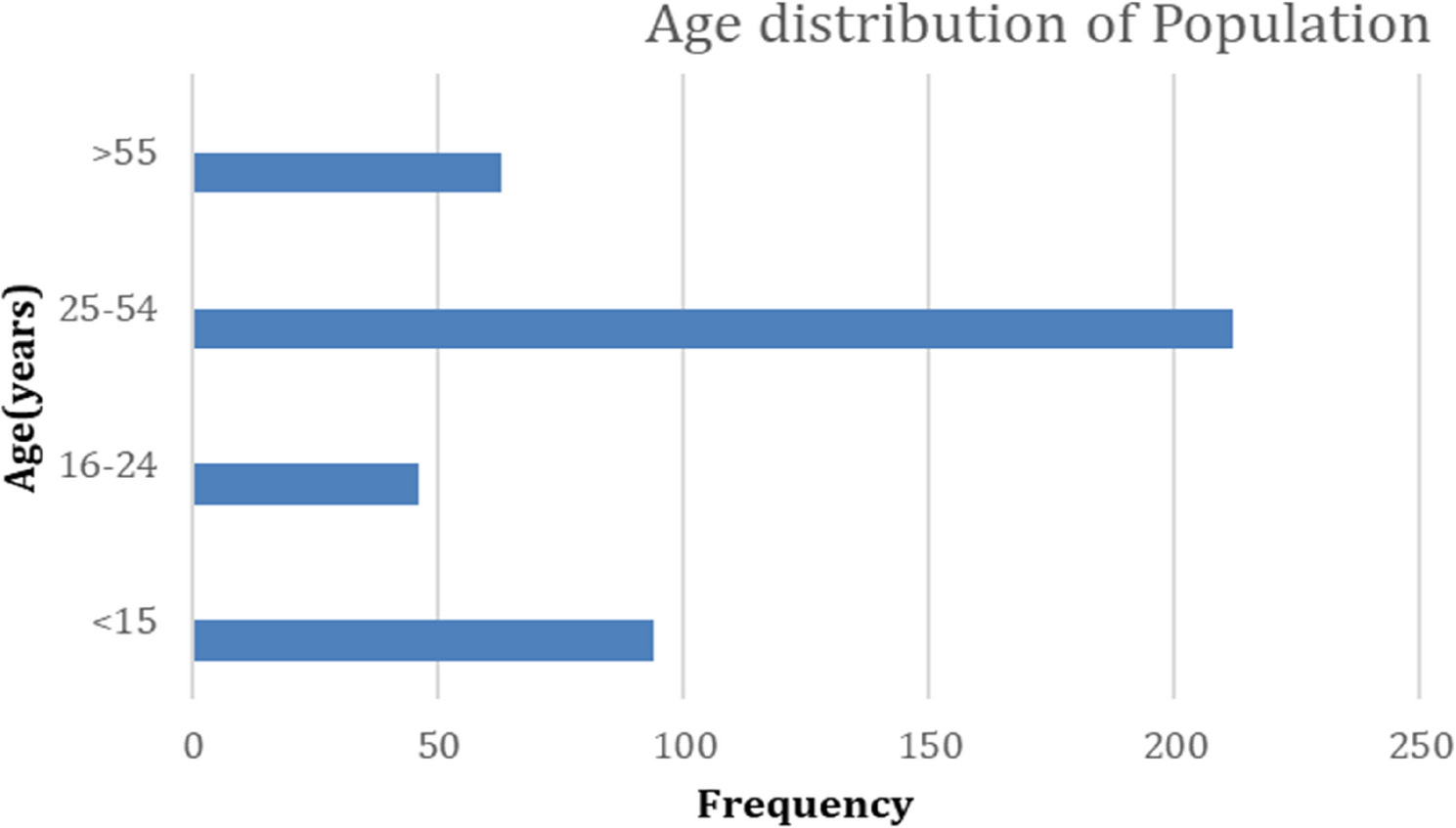
Regarding demographic factors, gender was not significantly associated with hantavirus seropositivity. Among the 21 positive cases, 42.9% were male and 57.1% were female, which contrasts with most studies, where a higher proportion of males are affected [14]. A significant difference was found in age groups, with most positive cases occurring in individuals under 10 years and over 61 years. While hantavirus infections in most regions, including the Americas, Asia, and Europe, primarily affect adults, studies from Iran and Barbados have highlighted the occurrence of pediatric cases, suggesting varying age distributions of hantavirus infections across different regions [28].
Clinical and laboratory factors in probable hantavirus patients
Most hantavirus-positive patients (76.2%) did not require special care, and only 14.3% required intensive care. Two deaths were reported, corresponding to a mortality rate of 9.5%, which is slightly lower than that observed in similar studies. Fever was present in all positive cases, while other symptoms such as cough, myalgia, and arthralgia were reported in a subset of patients. The absence of severe symptoms in most cases suggests that the majority of infections were mild. Chest X-rays revealed pulmonary involvement in three patients, and renal failure was diagnosed in two patients, with symptoms consistent with both Hemorrhagic Fever with Renal Syndrome (HFRS) and Hantavirus Pulmonary Syndrome (HPS). These findings align with recent studies conducted in Sri Lanka, indicating that Hantavirus can present with a range of clinical manifestations [11]. Without specific efficient antiviral therapy, these patients were managed symptomatically with supportive care.
Regarding laboratory results, thrombocytopenia was observed in 8 out of 17 positive cases, although it was not a common finding across all patients. Leukocytosis and elevated hematocrit were observed in a few patients; however, none of the cases showed a significant increase in hematocrit. These laboratory abnormalities, which are typically seen in the later stages of the disease, may have been missed because testing was conducted during the early or mild stages of infection [29]. Additionally, elevated ALT, AST, and CRP levels were noted in most positive cases, consistent with findings from a similar study conducted in Indonesia. These markers are indicative of liver involvement and systemic inflammation, reinforcing the need for comprehensive testing during the clinical evaluation of patients [30, 31].