The clinical significance of occult HBV carriers frequently identified in individuals who are HBsAg-negative/HBcAb-positive, is well-documented [13, 15]. However, the increasing scarcity of available donors necessitates the expanded utilization of grafts from HBcAb-positive donors, particularly in regions with intermediate to high HBV endemicity. Although considerable evidence suggests that HBcAb-positive donor grafts carry a potential risk of transmission HBV infection following liver transplantation [5, 6] limited research has focused on quantifying the specific risk of de novo HBV infection in pediatric patients associated with the use of those grafts. To address those knowledge gaps, we conducted a comprehensive prospective study to specifically evaluate the risk associated with HBcAb-positive liver grafts in pediatric recipients.
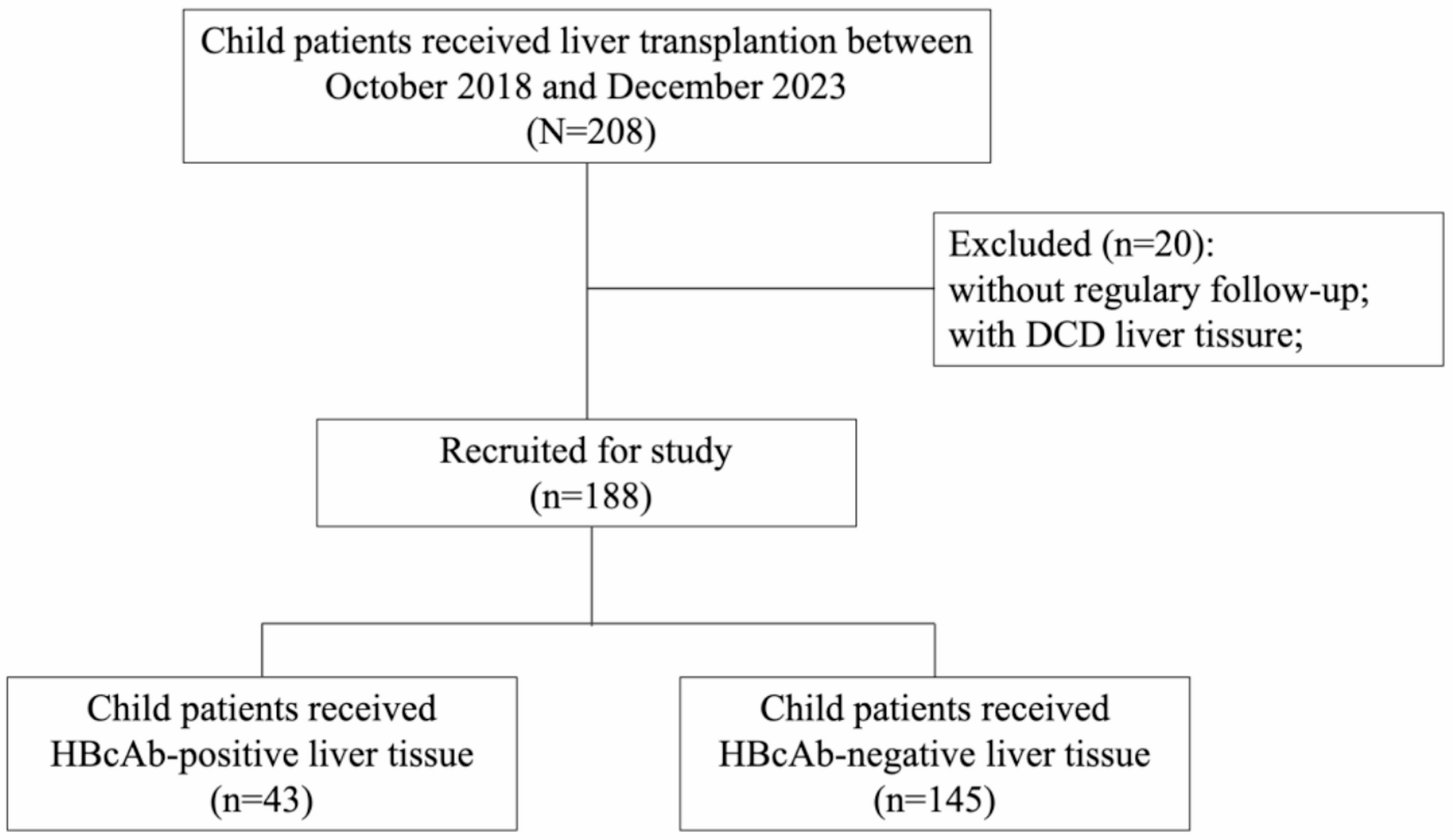
In this study, we had embedded within a prospective observational cohort of living donor liver transplantations, encompassing all consecutive transplantations performed over a 6-year period in China with a relatively high prevalence of HBcAb-positive individuals in the general population. In our cohort, a total of 5.3% (10 out of 188) of pediatric patients developed HBV infection post-transplantation. Notably, the incidence of de novo HBV infection was significantly higher in children receiving HBcAb-positive grafts (16.3%, 7 out of 43) compared to those receiving HBcAb-negative grafts. This was evidenced by a 15% difference in the 2-year cumulative incidence rate of HBV activation between the two groups. The status of HBV infection in pediatric patients prior to liver transplantation remains unclear. To further ascertain whether post-transplant HBV infection results from the transmission of HBV from liver donors or the reactivation of a previous infection in recipients, liver tissue from pediatric patients was utilized as the detection sample for diagnosing occult HBV infection (OBI). Previous research has demonstrated that ddPCR offers greater sensitivity and accuracy in detecting low DNA concentrations compared to conventional PCR technologies [12]. In this study, we employed a sensitive PCR system based on ddPCR technology to analyze liver DNA extracts from recipients with de novo HBV infection. Among the seven liver samples analyzed, only one tested positive (patient #3), while the remaining samples were negative. These findings suggest that de novo HBV infection in pediatric patients following liver transplantation is primarily attributable to HBV transmission from liver grafts, with a significantly increased risk of HBV transmission to pediatric recipients when transplanting with HBcAb-positive liver grafts. It is also clinically relevant that all of these patients were negative for HBcAb at the initial diagnosis of infection. This likely reflects the early serological window of acute infection, a period prolonged by the potent immunosuppression and inherent immune immaturity of this young cohort.
A particularly challenging finding was the occurrence of de novo HBV infection in three patients (#3, #5, and #6) who were HBcAb-negative and received grafts from HBcAb-negative donors. Our analysis of their native liver tissues provides insight into these complex cases. For patient #3, the detection of both total HBV DNA and cccDNA in the pre-transplant liver tissue, despite negative serology, provides strong evidence for a pre-existing seronegative OBI in the recipient. The subsequent infection was therefore most likely due to the reactivation of this latent virus under immunosuppression. The interpretation for patients #5 and #6, whose pre-transplant liver tissues were negative by ddPCR, is more complex and highlights two critical, non-mutually exclusive possibilities. One hypothesis is that these recipients also had seronegative OBI, but the viral load was below the ddPCR detection limit or was patchily distributed within the liver, leading to a false-negative result from the sampled tissue. Alternatively, the infection could have been transmitted from the HBcAb-negative donors. It is well-documented that a small fraction of HBcAb-negative individuals can harbor seronegative OBI and act as infectious sources [16,17,18]. While we cannot definitively determine the origin of infection for these two patients, their cases underscore an important clinical reality: the risk of HBV transmission or reactivation is not entirely eliminated even in “HBcAb-negative to HBcAb-negative” transplant settings. This finding warrants consideration in future risk assessment and management strategies.
The estimated elevated hazard ratio for de novo HBV infection associated with transplantation from HBcAb-positive donors demonstrated temporal variability. Specifically, the risk was negligible in the early post-transplantation period and reached its peak approximately one year (43 weeks) after transplantation. This pattern contrasts with findings in adult recipients, as noted in previous studies [19]. Such a discrepancy may suggest subtle interactions between HBcAb positivity and other concurrent protective factors that enhance the recipient’s health during the first year post-transplantation. Moreover, while prior research has indicated a negative impact of HBcAb-positive liver donors on graft survival [20] we observed no graft loss among pediatric patients who received HBcAb-positive livers. It is important to highlight that all participants in this study were children, with the majority being younger than one year old. Their distinct immune status and underlying conditions may have contributed to this divergent outcome, potentially through mechanisms that merit further investigation.
A noteworthy finding was the high pre-transplant HBcAb prevalence (22.3%) in our young cohort. This observation is critical: unlike in adult transplantation where recipient HBcAb signifies past exposure and is a major risk factor for de novo HBV infection [3] in our infant cohort, it more plausibly reflects the passive transfer of maternal IgG antibodies, not their own immune history. This phenomenon is common in HBV endemic regions [21,22,23]. Consequently, it did not emerge as an independent predictor of transmission in our analysis. This key distinction shifts the focus of protection away from the non-prognostic HBcAb status and squarely onto the establishment of a functional immune defense, for which hepatitis B vaccination is the important. However, our study reveals a significant gap in this strategy. While nearly all infants received the first vaccination dose at birth, the progression of their underlying liver disease frequently disrupted the subsequent immunization schedule. The second dose was often delayed or omitted due to jaundice and clinical instability, and the third was commonly missed as children were undergoing or recovering from transplantation, resulting in an incomplete active immune response for most patients. This common pattern of immunization failure, coupled with the unreliability of HBcAb as a risk marker, leaves this vulnerable population in a precarious position and highlights the urgent need for optimized prophylactic strategies.
Our findings highlight a critical dilemma in pediatric liver transplantation. While current guidelines for adult recipients strongly advocate for prophylactic strategies against HBV transmission from HBcAb-positive grafts, specific, evidence-based recommendations for children remain conspicuously absent [24, 25]. This lack of guidance directly contributed to the clinical reality observed in our study: specific anti-HBV prophylaxis was applied inconsistently and infrequently. The absence of a mandated protocol meant that decisions were left to individual clinical judgment, often in a context of uncertainty regarding the true level of risk. This real-world scenario, however, does not weaken our study’s conclusions—it strengthens them. Our analysis demonstrates a significant risk of de novo HBV infection (16.3%) even within a cohort where some sporadic prophylaxis may have occurred. This underscores that incomplete pre-transplant vaccination alone is an insufficient safeguard. In this context, our data on the protective effect of high HBsAb titers (≥ 100 mIU/mL) becomes particularly valuable. The finding that recipients with higher HBsAb levels had a significantly lower infection rate (3% vs. 14%) may provide a tangible, evidence-based direction for future pediatric-specific guidelines. It suggests that maintaining robust HBsAb levels, either through a completed vaccination series or other passive immunization strategies, may be a important method in mitigating the transmission risk from HBcAb-positive grafts in children. Furthermore, the observed pattern of declining HBsAb titers preceding viral breakthrough strongly suggests that routine post-transplant monitoring of HBsAb levels could serve as a valuable clinical strategy. Such monitoring would enable timely interventions, like booster vaccinations or passive immunization, to maintain protective immunity in these high-risk patients. In addition to these immune-based strategies, the use of antiviral prophylaxis with nucleos(t)ide analogues (NAs) should be considered, particularly for the highest-risk subgroups identified in our study, such as recipients with low or undetectable baseline HBsAb titers. While NAs are the standard of care in adult settings, their optimal use in children—including patient selection, timing, and duration of therapy—requires further investigation to establish clear, evidence-based guidelines for pediatric practice.
Our study has several limitations inherent to its design. Firstly, our study is limited by its median follow–up period of two years. While this duration was sufficient to identify the peak risk of transmission within our cohort, it is not long enough to evaluate critical long-term clinical outcomes, such as the development of chronic hepatitis or graft loss. Continued follow-up of this cohort will be crucial to address these important questions. Secondly, as a real-world study, the follow-up frequency for HBV marker surveillance was not rigidly fixed, which may have led to delays in the detection of de novo infection in some cases. Thirdly, our monitoring strategy, reflective of real-world practice in many resource-limited settings, had inherent limitations. Our approach relied predominantly on serological markers, which may miss early viral replication. This was compounded by the fact that the HBV DNA assay used for follow-up had a relatively high limit of quantitation (400 IU/mL). Collectively, these factors limited our ability to detect low-level viremia and may have led to an underestimation of the true infection rate. Finally, this cohort study is constrained by its single-center design and a relatively small sample size, which may limit the statistical power and the generalizability of our findings to other populations. Despite these limitations, our study provides robust evidence that significantly contributes to the existing body of knowledge. It highlights the substantial risk of HBV transmission from HBcAb-positive grafts even under real-world surveillance conditions and underscores the necessity for developing standardized prophylactic and monitoring strategies.
In conclusion, our findings indicate that liver transplantation using HBcAb-positive grafts poses a substantial risk of de novo HBV infection in pediatric recipients. Although previous research has predominantly focused on adult populations, our study emphasizes that the clinical impact of HBcAb-positive grafts on pediatric patients warrants equal attention. In this context, the potential occurrence of seronegative OBI also remains a significant concern. Strategies designed to rapidly elevate HBsAb levels may effectively mitigate this risk. Moreover, the careful selection of appropriate prophylactic measures and the determination of optimal timing for post-transplant HBV monitoring could be critical for improving outcomes in pediatric liver transplant recipients. Future studies should aim to refine these approaches and further elucidate the long-term clinical implications of using HBcAb-positive grafts in pediatric patients.