Patient inclusion and characteristics
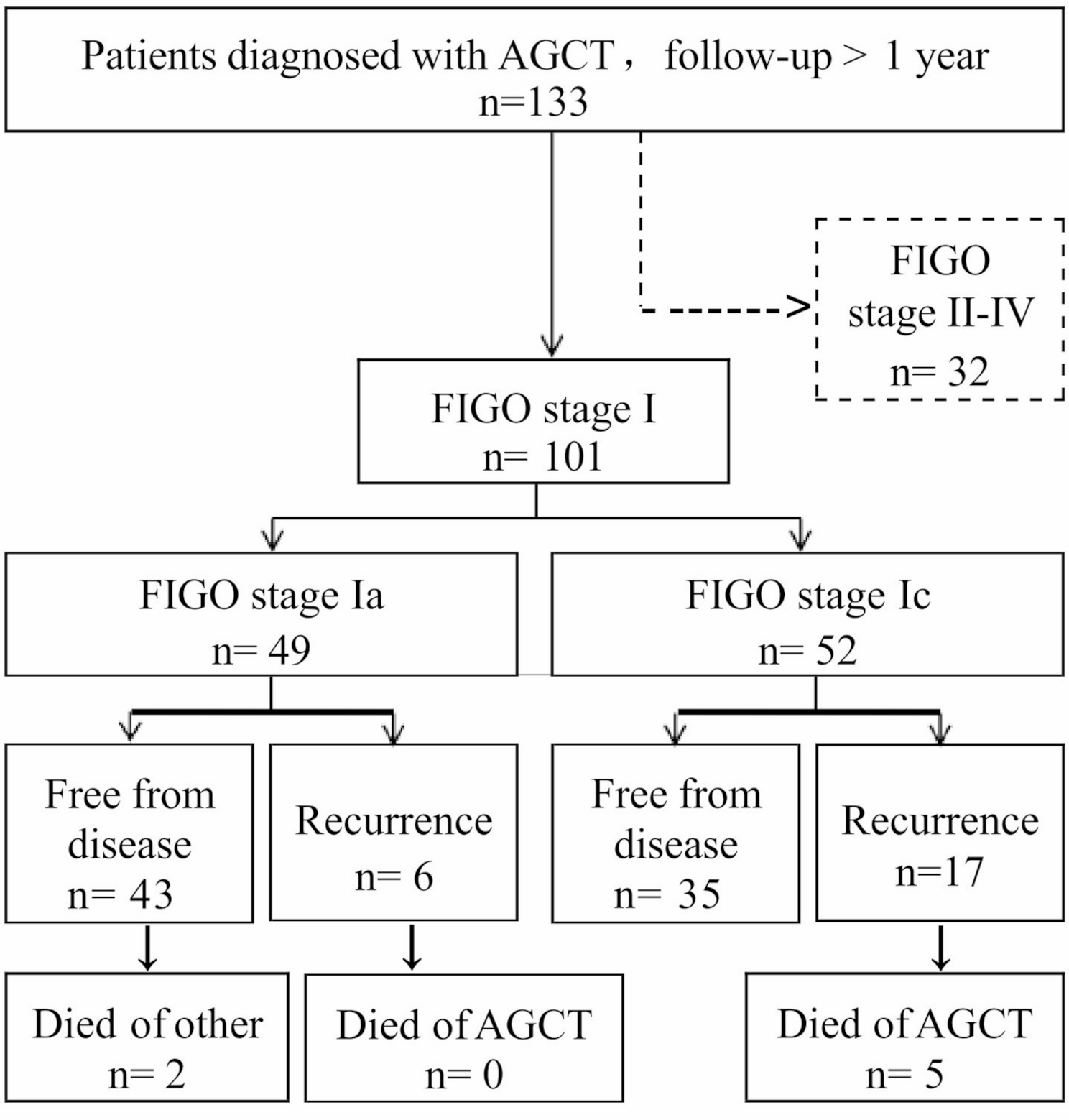
A total of 133 patients with AGCT were identified by comprehensive search of medical records. Among them, 101 (75.9%) patients were diagnosed with stage I disease, including 49 (36.8%) stage Ia and 52 (39.1%) stage Ic patients. With a median follow up time of 47.7 months (range 4.0 to 246.5 months), a total of 23 (22.7%) patients relapsed including 6 (12.2%) stage Ia and 17 (32.7%) stage Ic patients., 5 (4.9%) patients died of AGCT, and 2 (1.9%) patients died of other causes. All patients were followed up more than one year except for those who died within one year. The managements and outcomes of stage I patients were shown in Fig. 1.
Flow chart of managements and outcomes of patients with stage I AGCT
These 101 patients, according to the timing and basis of pathological diagnosis, were categorized into the following three groups: preoperative consultation of paraffin section examination (pre-cPSE) group, intraoperative frozen section examination (intra-FSE) group, and postoperative paraffin section examination (post-PSE) group. There were 18 cases in the pre-cPSE group, who underwent incomplete initial surgery at outside hospitals. Among the remaining 83 cases, intra-FSE findings were consistent with AGCT in 49 cases. The remaining 34 cases, which were reported as suspicious for or could not exclude AGCT intraoperatively, were ultimately diagnosed by post-PSE. The Chi-square test was performed to assess whether the surgical approach (Open vs. Laparoscopic) was influenced by a confirmed or presumed diagnosis (pre-cPSE group vs. intra-FSE group and post-PSE group), and the results revealed no association between the two factors (χ2 = 2.989, p = 0.084), indicating that obtaining a preoperative AGCT diagnosis was not significantly associated with the choice of surgical approach (shown in Table S1).
For those diagnosed with stage I disease, the median age at diagnosis was 45 years old (range 22 to 71 years). All patients achieved optimal cytoreduction. Open and laparoscopic surgery was performed in 68 (67.3%) and 33 (32.7%) patients, respectively. Conservative and radical surgery was performed in 37 (36.6%) and 64 (63.4%) patients, respectively. Forty-two (41.6%) patients received lymphadenectomy, including 21 cases with PLND and 21 cases with both PLND and PALND, the average number of lymph nodes dissected was 28 (range 10–62). However, only one patient who had second cancer history occurred lymphatic metastasis, which was confirmed by pathologists as stage IIIc endometrial adenocarcinoma. More details of the clinicopathological characteristics of stage I AGCT patients were shown in Table 1.
Survival and recurrence
The 5-year and 10-year cancer specific survival (CSS) rates for all stage I patients were 97% and 90%, respectively; while the 5-year and 10-year disease-free survival (DFS) rates were 84% and 53%, respectively. There was a significant difference between stage Ia and stage Ic patients in terms of 10-year CSS and DFS rates (100% vs. 83%, P = 0.040; 66% vs. 44%, P = 0.033). The median DFS for all stage I and stage Ic patients were 135.0 months and 112.7 months. During follow-up, less than 50% stage Ia patients relapsed, so the median DFS could not be calculated. CSS and DFS curves were shown in Fig. 2, indicating a significant survival advantage for both CSS and DFS of stage Ia disease compared with stage Ic.
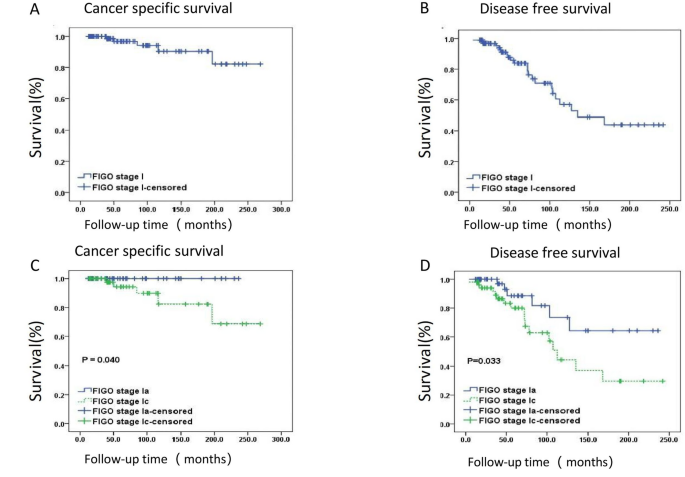
Kaplan-Meier curves of CSS and DFS according to disease stage. (A) CSS of stage I, (B) DFS of stage I, (C) CSS according to disease substages (stage Ia vs. Ic), (D) DFS according to disease substages ( stage Ia vs. Ic)
The median time to relapse was 72.3 months for these relapsed patients, including 4 (17.4%) patients with recurrence at 0–3 years, 7 (30.4%) patients at 3–5 years, and 12 (52.2%) patients after 5 years. The latest recurrence was observed 14 years after primary treatment. At first relapse, the anatomic positions were mainly located in pelvic cavity (14/23, 60.9%), abdominal cavity (3/23, 13.0%), retroperitoneum (2/23, 8.7%), adnexa (1/23, 4.3%) and multiple positions (3/23, 13.0%). All patients with recurrent tumor received surgical excision and chemotherapy except for one patient who refused chemotherapy. Two patients with retroperitoneal recurrence received radiotherapy. The median follow-up time after recurrence was 54.3 months (range 3.6-196.3 months), and 5 deaths were observed. The prognosis of recurrent AGCT was generally favorable with a five year overall survival rate of 71.9%. Details of patients with recurrence are given in Table S2 .
Prognostic factors
Using log rank test, we found that advanced FIGO substage (P = 0.033), tumor rupture(P = 0.022), tumor size > 5 cm (P = 0.021), conservative surgery (P = 0.002) and laparoscopic surgery (P = 0.002) were significantly associated with a decreased DFS (shown in Table 2). However, age, menopausal status, parity, comorbidity, second cancer history, symptoms at diagnosis, ascite, endometrial pathology, salvage surgery and lymphadenectomy were not associated with patients’ DFS (P > 0.05).
To further determine the independent prognostic factor in these patients, univariate and multivariate analysis were performed (shown in Table 2). Univariate analysis showed that FIGO substage (HR: 2.650, P = 0.041), tumor rupture(HR:2.595, P = 0.027), surgical extent (HR: 3.577, P = 0.003) and surgical approach (HR: 3.699, P = 0.004) were prognostic factors for patients’ DFS. However, multivariate analysis showed that only surgical extent (HR: 2.738, P = 0.034) was an independent prognostic factor for DFS of these patients.
Given the significant prognostic value of surgical extent in AGCT, we categorized patients into two groups: those who underwent conservative surgery and those who underwent radical surgery. To further evaluate their impact on survival outcomes and address baseline imbalances, we applied IPTW to this retrospective dataset, which resulted in well-balanced covariates between the two surgical groups (shown in Table S3). After adjustment, radical surgery was consistently associated with improved DFS compared to conservative surgery (conservative vs. radical surgery HR: 3.561, P = 0.027).
Survival impact of surgical modalities on patients with different FIGO substage or tumor size
To identify optimal candidates for radical surgery among patients with stage I AGCT, we performed subgroup analyses based on FIGO substage and tumor size—two key clinical decision-making factors. We found that surgical extent had no significant impact on DFS of stage Ia patients (conservative vs. radical surgery HR: 1.747, P = 0.538). However, for stage Ic patients, conservative surgery was significantly associated with worse DFS compared with radical surgery (HR: 4.021, P = 0.007). Notably, similar result was also observed in the comparison between laparoscopic and open surgery (HR: 2.926, P = 0.035). Corresponding Kaplan-Meier curves were shown in Fig. 3A-D.
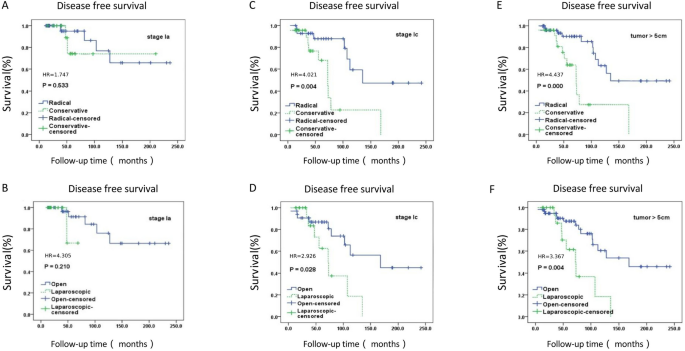
Subgroup analysis of surgical modalities. (A) Surgical extent (stage Ia), (B) Surgical approach (stage Ia), (C) Surgical extent (stage Ic), (D) Surgical approach (stage Ic), (E) Surgical extent (tumor > 5 cm), (F) Surgical approach (tumor > 5 cm)
Taken that tumor size is an important factor for the decision-making of surgical modalities, a subgroup analysis was performed. For patients with tumor ≤ 5 cm, surgical extent and surgical approach had no impact on DFS (no recurrence in any subgroup). However, for patients with tumor > 5 cm, conservative surgery was significantly associated with decreased DFS compared to radical surgery (HR:4.437, P = 0.001), and similar result was observed in the comparison between laparoscopic and open surgery (HR: 3.367, P = 0.006). Corresponding Kaplan-Meier curves were shown in Fig. 3E-F.