Respondents’ professional background and socio-demographics
As part of the data processing, two respondents were excluded because their answers indicated they were not part of the target population. Twenty-nine questionnaires were excluded since only socio-demographic information had been provided.
A total of 60 physicians either specialized in oncology or another medical or surgical discipline with a focus on oncological patients (e.g. neuro-oncology, thoracic oncology) participated in the survey. Most participants stated to be specialized in hematology/oncology (N = 42/60; 70.0%) and were permanent members of an oncological tumor board (N = 46/60; 76.7%).
The majority was between 36 and 55 years old (N = 42/60; 70.0%) and more than a third had 21 or more years of professional experience (N = 22/60; 36.7%). Additionally, more than half of the physicians worked as a chief or senior physician (N = 37/60; 61.7%) (Table 1).
LOT: Definition and relevance
The vast majority of physicians (N = 57/60; 95.0%) agreed (fully or somewhat) that LOT is a self-contained therapy concept, based on various patient and tumor characteristics, including different therapy modalities, and aims at specific treatment goals. Although there was a relatively strong consensus regarding the definition of the LOT-concept (GMD = 0.28, 95%-CI = [0.21; 0.35]), regarding complex or rare situations, more than half of the respondents (N = 32/60; 53.3%) disagreed that there are clear-cut, uniform and commonly used criteria for determining LOTs (GMD = 0.52, 95%-CI = [0.42; 0.61]). While more than three quarters (N = 51/59; 86.5%) of physicians considered LOT as extremely relevant (defined as an answer of highly relevant or relevant) concept in everyday clinical practice (GMD = 0.41, 95%-CI = [0.32; 0.49]), half of respondents (N = 30/60; 50.0%; GMD = 0.38, 95%-CI = [0.31; 0.44]) deemed it as highly relevant for research purposes.
Stage of disease and treatment intention
Most respondents considered LOT as a relevant concept across various disease stages, i.e. from early stages to locally advanced or metastatic disease (N = 41/60; 68.3%). However, opinions varied highly (GMD: 0.62, 95%-CI = [0.49; 0.76]).
A majority of respondents (N = 44/60; 73.3%) considered LOT relevant for both palliative and curative treatment intentions. Nevertheless, differing opinions on this question, led to a low level of agreement in responses (GMD: 0.54, 95%-CI = [0.40; 0.65]).
Change of LOT
Most respondents stated that primary tumor progression (N = 58/60; 96.7%; NE: 0.21, 95%-CI = [0.04; 0.52]), metastasis occurrence (N = 55/60; 91.7%; NE: 0.41, 95%-CI = [0.18; 0.69]), disease recurrence (N = 52/60; 86.7%; NE: 0.57, 95%-CI = [0.32; 0.80]), and relevant therapy side-effects (N = 46/60; 76.7%; NE: 0.78, 95%-CI = [0.57; 0.94]) indicated changing LOTs.
Additionally, more than half of the respondents reported that discontinuation of all previously administered drugs (N = 37/54; 68.5%) equaled a change of LOT. A high NE-value of 0.90 (95%-CI = ([0.71; 0.99]), however, indicated strong disagreement. Furthermore, they predominantly stated that replacing previously administered drugs with different, non-equivalent drugs (N = 47/54; 87.0%; NE: 0.56, 95%-CI = [0.30; 0.81]) was a common practice for changing LOT. The majority of the surveyed physicians (N = 33/54; 61.1%) agreed that adding one or more new drugs to an existing drug regimen is an indicator of changing LOT. However, for this statement, analysis revealed a strong dissension (NE: 0.96, 95%-CI = [0.83; 1.00]) (Table 2). The frequencies, percentages and consensus metrics of all events and measures for a change of LOT are detailed in Table 2.
For all events and measures regarding the change of LOT, the proportions of affirmative responses and CP CIs are detailed and illustrated in Figure D.1 and Table D.1 in Additional file D.
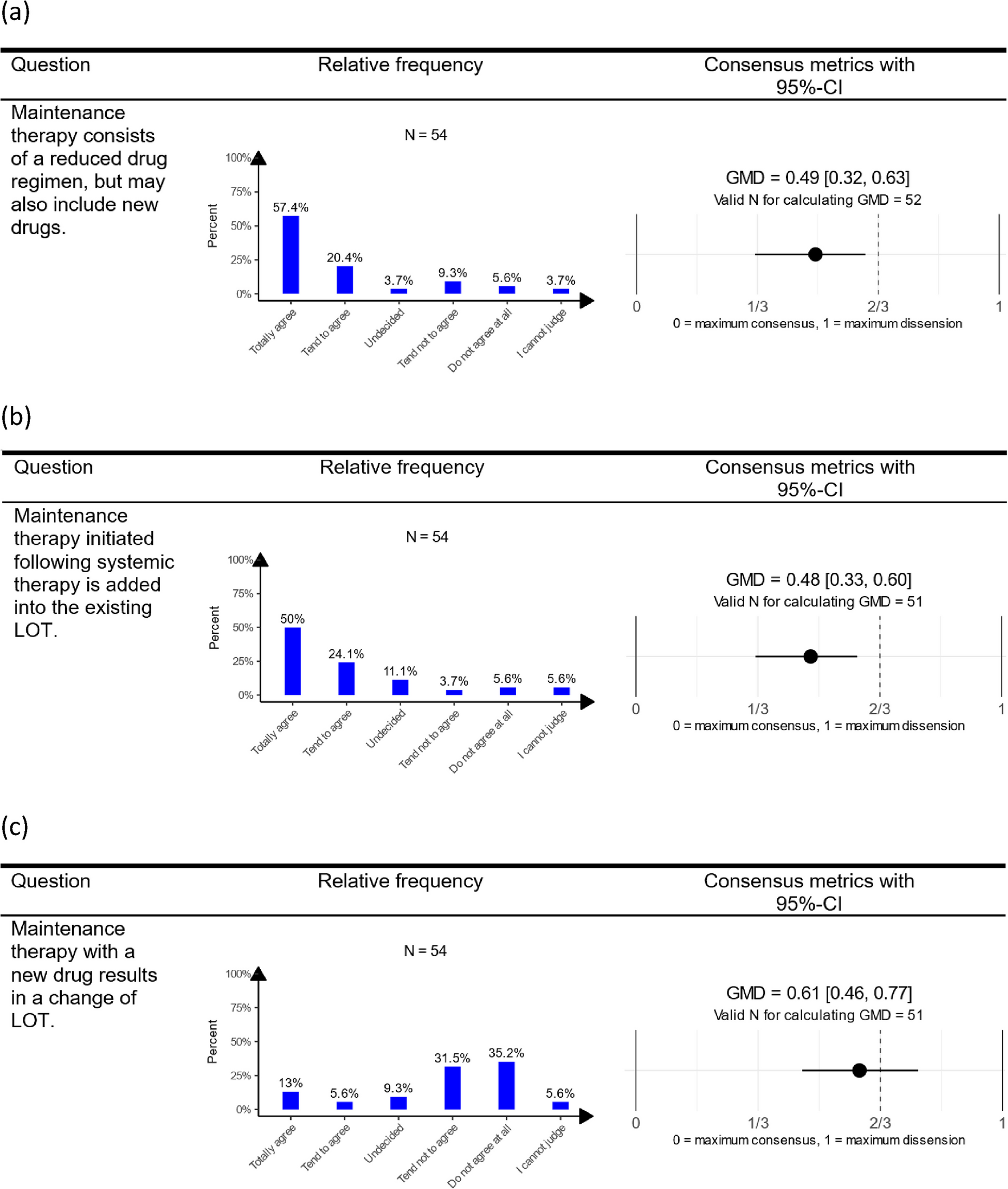
Descriptive and consensus results (95%-CIs) regarding maintenance therapy with reduced drug regimen or new drugs (a), maintenance therapy initiated after systemic therapy (b) and maintenance therapy with new drug as change of LOT (c). Note: A value for GMD of (0) corresponds to unanimity, (2/3) to maximal uncertainty (i.e., uniform distribution across answers), and (1) to maximal dissension (i.e., equally sized groups opining at opposite ends of the spectrum). The standardization transformation serves to make GMD values comparable across questions with different numbers of possible answers. The response categories “I cannot judge” and “I am unsure” were excluded as indeterminate responses for calculating GMD. This leads to a little lower N for calculating the consensus metrics in comparison to the N for descriptive statistics. For the presentation in the table, a short version of the questions was used. An overview of the short versions with the assigned detailed formulation for all questions is given in Table B1 in Additional file B. Abbreviations: CI, confidence interval; GMD, Gini mean difference; LOT, line of therapy
Maintenance therapy
A great part of the respondents (N = 42/54; 77.8%) agreed or tended to agree that maintenance therapy typically involves a reduced regimen of previously administered drugs but may also include new drugs. However, there was considerable heterogeneity across survey participants on this statement (GMD: 0.49, 95%-CI = [0.32; 0.63]). The majority (N = 40/54; 74.1%; GMD: 0.48, 95%-CI = [0.33; 0.60]) agreed that reduced regimen, initiated following systemic therapy, is part of an existing LOT. Conversely, two-third of physicians (N = 36/54; 66.7%; GMD: 0.61, 95%-CI = [0.46; 0.77]) did not consider the introduction of a new drug in systemic therapy as indicative of a LOT change. The results of all descriptive statistics and GMD values including CIs for all questions regarding maintenance therapy are visualized in Fig. 1.
Therapy modality
For most respondents, surgery (N = 20/54; 37.0%; GMD: 0.55, 95%-CI = [0.43; 0.64]) as well as radiotherapy (N = 23/54; 42.6%; GMD: 0.47, 95%-CI = [0.35; 0.57]) only partially constituted separate LOTs. A majority (N = 42/54; 77.8%; GMD: 0.36, 95%-CI = [0.17; 0.53]) approved that both radiotherapy and chemotherapy are essential to the LOT in cases of radiochemotherapy (Figure 2D in Additional file D).
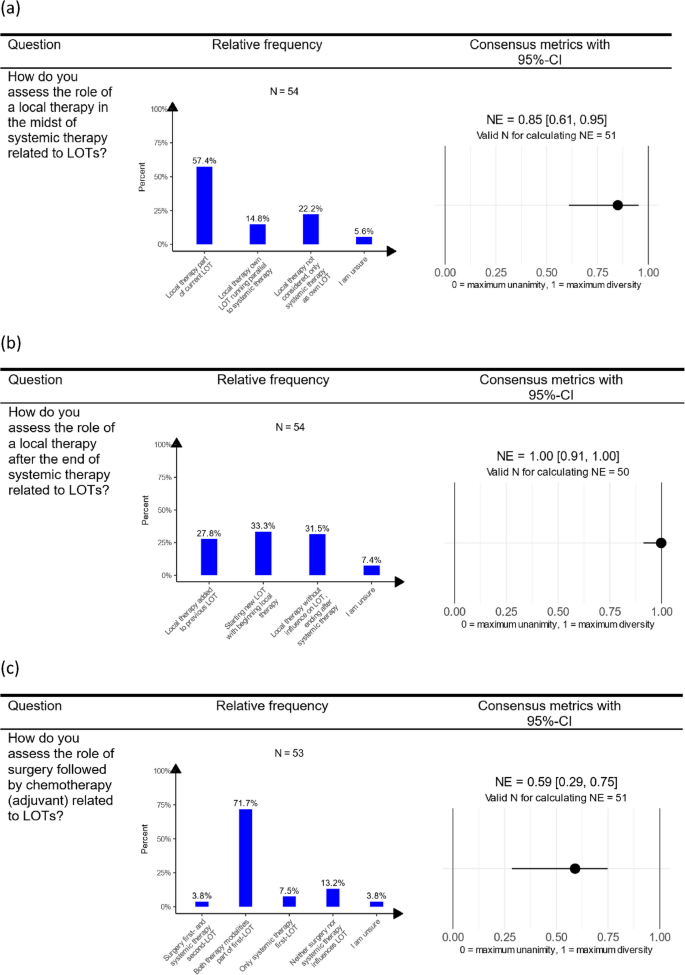
Descriptive and consensus results (95%-CIs) regarding local therapies in the midst of a systemic therapy (a), local therapies after the end of a systemic therapy (b) and surgery followed by chemotherapy (adjuvant) (c). Note: A value for NE of (0) corresponds to unanimity, and (1) represents maximal diversity of opinions. The confidence interval for the NE regarding local therapy after the end of systemic therapy now includes the value (1), indicating that a hypothesis at the 5% significance level cannot be reject. This suggests that there is maximum disagreement about local therapy after the end of systemic therapy. The response category “I am unsure” was excluded as indeterminate response for calculating NE. This leads to a little lower N for calculating the consensus metrics in comparison to the N for descriptive statistics. For the presentation in the table, a short version of the questions was used. An overview of the short versions with the assigned detailed formulation for all questions is given in Table 1B in Additional file B. Abbreviations: CI, confidence interval; LOT, line of therapy; LOTs, lines of therapy; NE, normalized entropy
Respondents further indicated that local therapy during systemic therapy is part of the ongoing LOT (N = 31/54; 57.4%; NE: 0.85, 95%-CI = [0.61; 0.95]). Opinions varied on local therapy post-systemic therapy: 27.8% (N = 15/54) considered local therapy as part of the previous LOT, 33.3% (N = 18/54) viewed it as the start of a new LOT, and 31.5% (N = 17/54) believed it does not impact the LOT status (NE: 1.00, 95%-CI = [0.91; 1.00]) (Fig. 2).
Therapy interruption
In cases where therapy was interrupted for either 30 or 180 days across low- and high-grade tumors, most respondents indicated that the LOT remains unchanged post-interruption (30 days, low-grade: N = 50/53; 94.3%; GMD: 0.11, 95%-CI = [0.00; 0.24]; 180 days, low-grade: N = 30/53; 56.6%; GMD: 0.65, 95%-CI = [0.49; 0.92]; 30 days, high-grade: N = 44/53; 83.0%; GMD: 0.31, 95%-CI = [0.11; 0.49]; 180 days, high-grade: N = 24/52; 46.2%; GMD: 0.83, 95%-CI = [0.60; 0.99]).
However, if there was an interruption between two different therapies, either because of a therapy-free period in between (N = 46/52; 88.5%; GMD: 0.09, 95%-CI = [0.00; 0.19]) or due to progression or recurrence (N = 49/52; 94.2%; GMD: 0.14, 95%-CI = [0.00; 0.29]), most participants decided for a change of LOT (Table 3). All frequencies, percentages and consensus metrics for questions regarding the role of therapy interruptions for LOT are detailed in Table 3.
All non-standardized GMD-values for the various thematic blocks are listed in Table D.2 in Additional file D.