-
Twenty-five patients, 15 males and 10 females, with confirmed MDs and ocular involvement were enrolled in this study. Mean age at evaluation was of 47,2 ± 16.07 years (range 20–71 years), while mean age at disease onset was 22,56 ± 9.90 years (range 8–40 years). Mean time of disease was 24.64 ± 13.16 years. Twenty-two (88%) out of 25 patients had a PEO/PEO plus phenotypes, three (12%) of them a KSS. Regarding the genotype we found the following data: 10 patients (40%) reported single mtDNA deletion, 7 (28%) POLG variants [22], 5 (20%), SLC25A4 variants[23], 2 (8%) m.3243A > G [24] and 1 (4%) patient associated with TOP3A variant. [25]. As major ocular history not directly associated to the mitochondrial myopathy, a 22 years-old patient underwent cataract surgery in both eye at age of 10 for bilateral congenital cataract.
Visual acuity
Mean BCVA was 0.092 ± 0.125 LogMAR in right eye and 0.096 ± 0.149 LogMAR in left eye.
Lens and fundus evaluation
In 2/25 patients (8%) a cortico-nuclear cataract was detected, while 2/25 (8%) were pseudophakic.
Only one (4%) patient, affected by KSS, showed abnormalities of the macular RPE.
Ocular motility and angle of deviation
An exodeviation was found for far in 21 (84%) patients, 3 (12%) had a vertical deviation and 1 (4%) an esodeviation. Likewise, an exodeviation for near was found in 21 (84%) patients, 3 (12%) had a vertical deviation and 1 (4%) an esodeviation. In particular, 1 patient showed exodeviation for far and vertical deviation for near; 1 patient showed vertical deviation for far and esodeviation for near, and 1 patient had esodeviation for far and exodeviation for near. Mean far exodeviation (FAoD) was of −10,18 ± 11,23 prismatic diopters (PD), mean near exodeviation (NAoD) −17,33 ± 13,30 PD. The angle of deviation (AoD) value was classified as mild (< 8 PD), moderate (9–14 PD) and severe (> 15 PD). At cover test for distance, 15 patients (60%) showed a mild angle of squint, 3 (12%) moderate and 7 (28%) a severe angle for squint. At cover test for near, 7 patients (28%) showed a mild angle of squint, 8 (32%) moderate and 10 (40%) a severe angle for squint.
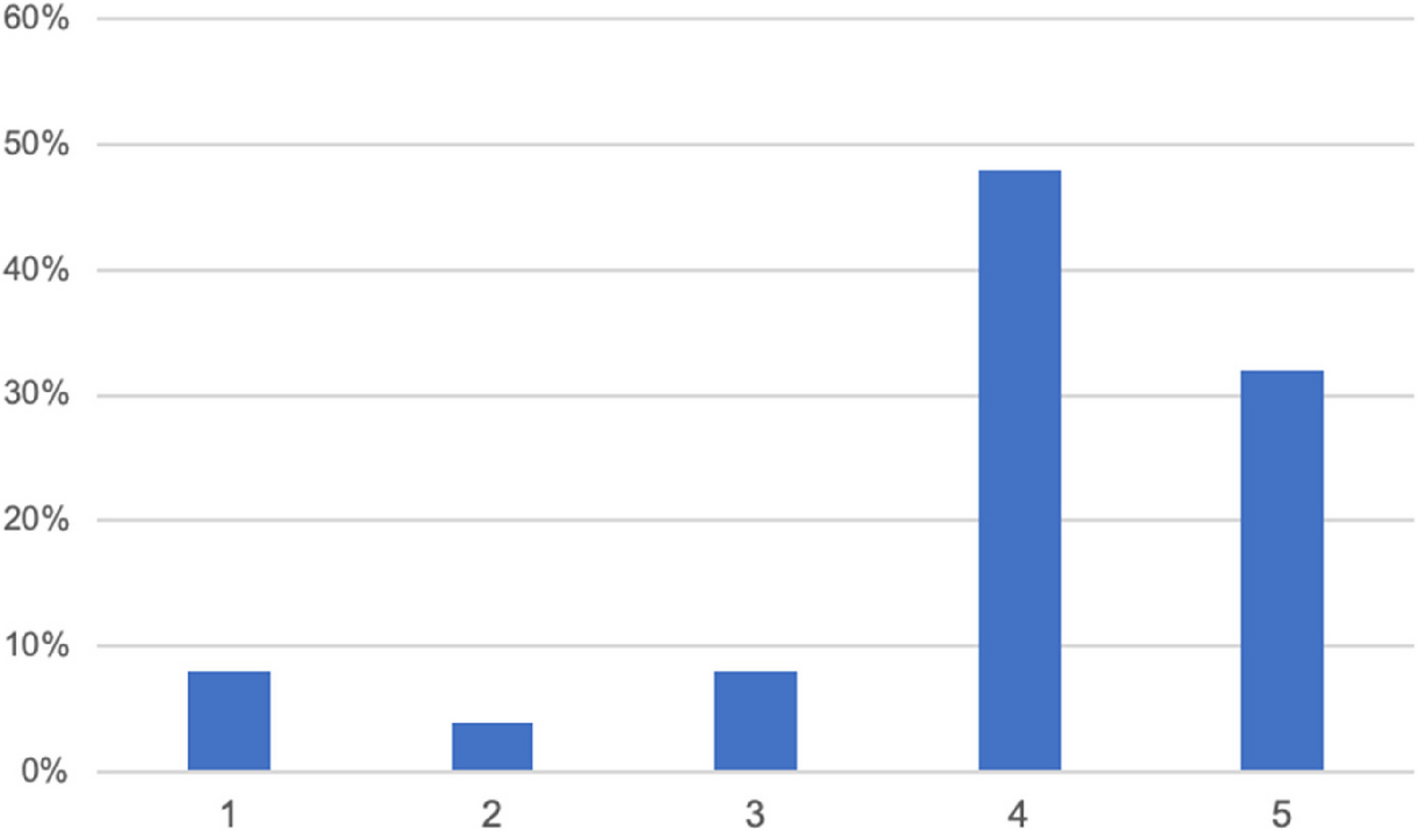
An ocular motility within the normal range (grade1), was observed in 2 of 25 patients (8%), a mild EOM impairment, (grade 2) in 1 of 25 patients (4%), a moderate impairment (grade 3) in 2 of 25 patients (8%), a severe EOM impairment (grade 4) in 12 of 25 patients (48%), and in 8 (32%) patients a complete ophthalmoplegia (grade 5) was observed. These results are reported in Fig. 1.
EOM impairment.1: normal motility, 2: mild impairment, 3: moderate impairment; 4: severe impairment; 5: complete ophthalmoplegia
Fusional vergence amplitudes
Convergence amplitudes for far (FCFAs) were within normal range in 5 patients (20%), low in 3 patients (12%), and absent in 15 patients (68%). Convergence amplitudes for near (NCFAs) were within normal range in 3 patients (12%), low in 4 patients (16%), and absent in 18 patients (72%).
Divergence amplitudes for far (FDFAs) were within normal range in 7 patients (28%), low in 3 patients (12%), and absent in 15 patients (60%). Divergence amplitudes for near (NDFAs) were within normal range in 4 patients (16%), low in 3 patients (12%), and absent in 18 patients (72%). General characteristic and ophthalmological features of the study population are shown in Tables 1 and 2.
Diplopia evaluation
We evaluated all patients in casual seeing conditions, at BSLs and WFDT.
Fifteen patients out 25 (60%) didn’t complain of double vision in casual seeing conditions, while 10 (40%) did. At far cover test 8 (53%) of the 15 patients who did not report diplopia had a manifest strabismus, and 1 (7%) patient had latent/manifest strabismus. At near cover test, 9 (60%) out of 15 patients had a manifest strabismus and 2 (13%) had a latent/manifest strabismus. The results are reported in Fig. 2.
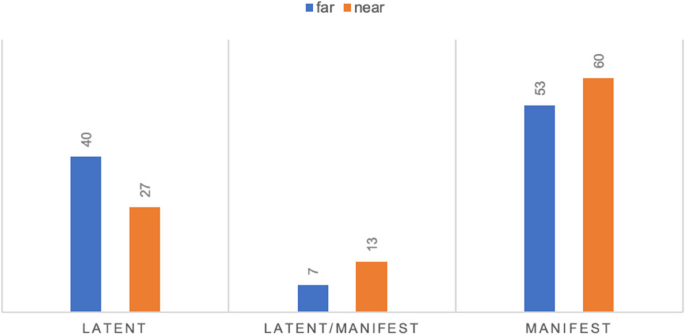
Distribution in percentage of strabismus among patients who didn’t complain of diplopia
At BSGs, when evaluated for far, 5 patients showed diplopia (20%), 8 suppression (32%), 3 suppression alternate to fusion (12%), 6 (24%) normal retinal correspondence (NRC) and 3 (12%) anomalous retinal correspondence (ARC)., When evaluated for near, 5 patients had diplopia (20%), 8 suppression (32%), 2 patients suppression alternate to fusion (8%), 3 suppression alternate to diplopia (12%), 6 patients NRC (24%) and 1 ARC (4%).
WFDT showed diplopia in 7 (28%) patients, suppression in 5 (20%) patients, suppression/fusion in 3 patients (12%), suppression/diplopia in 2 (8%) patients, NRC in 5 (20%) patients and ARC in 3 (12%) patients.
Furthermore, the response of patients with manifest or latent/manifest strabismus to the different sensorial tests was assessed.
Percentage of manifest strabismus with suppression mechanism are presented in Fig. 3.
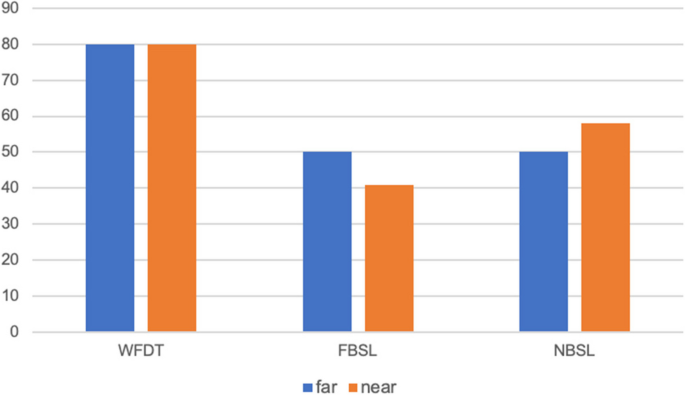
Patients in percentage with manifest strabismus with suppression mechanism at different functional tests
Moreover, we investigated how many patients who did not exhibit diplopia during normal vision had latent/manifest and manifest strabismus and evaluated how well these patients responded to sensory tests.
Of the 15 patients who did not complain of diplopia in casual seeing, for distance: 1 (36%) had latent/manifest strabismus, 8(53%) had manifest strabismus, the others were defined as latent. For near, however, 2 (13%) had latent/manifest strabismus and 9 (60%) had manifest strabismus. Only two (13%) patients who did not present diplopia with latent strabismus at far and manifest strabismus at near. The patient with latent/manifest strabismus for distance also had latent/manifest strabismus for near and a suppressive mechanism to both FBSL, NBSL and the WFDT. Of the 8(53%) patients with manifest strabismus for distance, 7 (88%) had manifest strabismus also at near and 1(12%) had latent/manifest strabismus at near. At the FBSL evaluation: 6 (75%) had a suppressive mechanism at distance and 2 (25%) had an ARC, while at near 6 (75%) had a suppressive mechanism, 1 (12.5%) NRC and 1 (12.5%) diplopia/suppression. At WFDT, on the other hand, 3 (37.5%) had a suppression mechanism, 3 (37.5%) had diplopia and 2 (25%) patients an ARC. For near, on the other hand, the two patients with latent/manifest strabismus both showed a suppression mechanism at WFDT and at FBSL and NBSL. Of the 9 patients with manifest strabismus at near, on the other hand, evaluated at FBSL: 5 (55%) had a suppression mechanism, 1 (11%) NRC, 2 (23%) ARC, 1 (11%) fusion/suppression. At the NBSL: 7 (78%) had suppression, 1 (11%) diplopia/suppression and 1(11%) ARC. At WFDT, 3 (33%) showed suppression, 2 (23%) ARC, 2 (23%) diplopia, 1 (11%) NRC and 1 (11%) fusion/suppression. The distribution of the population without diplopia is shown in Fig. 4 and Table 3. On the abscissas, from top to bottom for near strabismus, far strabismus and patients. On the ordinates, numbers from 1 to 6 to define: 1-NRC, 2-ARC; 3-suppression; 4-diplopia; 5-fusion/suppression; 6-diplopia/suppression.
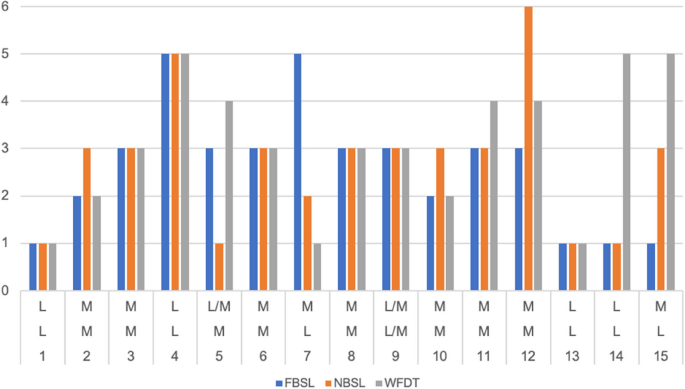
The distribution of the population without diplopia. On the abscissas, from top to bottom are reported latent (L), latent/manifest (L/M) and manifest (M) for near strabismus, far strabismus and patients. On the ordinates numbers from 1 to 6 to define: 1-NRC, 2-ARC; 3-suppression (S); 4-diplopia (D); 5-fusion/suppression (F/S); 6-diplopia/suppression (D/S)
Ptosis
Ptosis was reported in 22/25 patients (88%). Three (14%) of 22 patients had a monocular eyelid ptosis, whereas 19 cases (86%) had a binocular disease. The mean MRD value was of 1.8 mm (range −2/5 mm) in right eye (RE) and 1.35 mm (range −2/4 mm) in left eye (LE). Mean LF was 8.4 mm (range 2–20 mm) in RE and 7.4 mm (range 2–18 mm) in LE. Only 3 out 25 patients (12%) had a LF higher than 15 mm. Ten out 25 patients (40%) had a previous ptosis surgery, 5 of them received two or more surgeries, 2 cases were planned for a second surgery during the evaluation, and only 3 patients had undergone a single procedure. The surgeries performed were in 7 patients a levator aponeurosis resection/advancement (and in 4 cases was performed a surgical revision), one levator complex duplication with a subsequent levator resection, one frontal sling suspension; one patient has undergone a non-specified surgery.
Analysis of influence of age at onset, evaluation and elapsed time on disease phenotype
A statistical analysis was performed to correlate disease’s onset and type of mitochondrial myopathy. We compared the PEO/PEO plus group and the KSS using a t-test after analyzing the variables for normality with the Shapiro test. As expected, the difference in variance between the averages was statistically significant (p = 0.003); patients develop the PEO phenotype later than the KSS phenotypes. Two-sample t test with equal variances (PEO vs KSS) about disease’s onset is showed in Fig. 5.
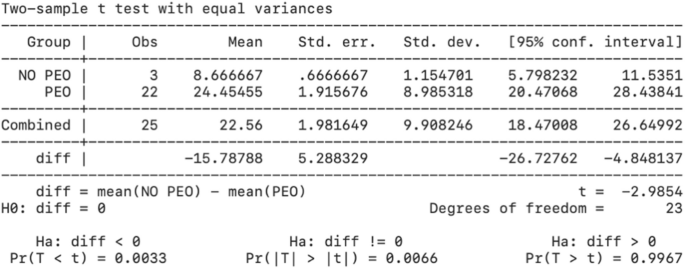
Two-sample t-test with equal variances (PEO vs KSS) about disease’s onset
The age at evaluation was also analyzed. The difference in variance between the means was statistically significant (p = 0.001): individuals with PEO come at the evaluation later, as showed in Fig. 6.
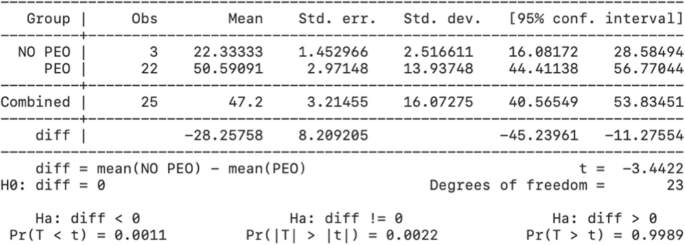
Two-sample t-test with equal variances (PEO vs KSS) about disease’s evaluation
To assess if the diplopia was onset disease-dependent, the same test was also conducted considering as variable the time of disease, i,e,. the difference between the age at evaluation and the age of onset, representing a not age-related time.
The results were not statistically significant (p = 0.06) (Fig. 7). Therefore, time-of-disease influences the age of onset of the disease, but not the presence of diplopia.
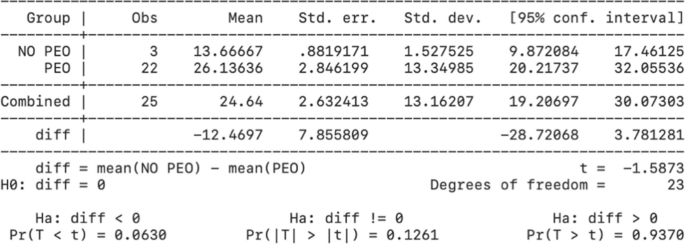
Two-sample t-test with equal variances (PEO vs KSS) about time of disease
Moreover, according to Hosmer and Lemeshow’s multivariable model construction, the variables identified as prospective predictors of diplopia at regression logistic (onset p = 0.018, time p = 0.165, angle of squint for near p = 0.172, ocular motility p = 0.199) did not provide statistically significant results (Table 4), indicating the presence of confounding factors.