Intraplacental choriocarcinoma (IC) represents an exceptionally rare variant of gestational trophoblastic neoplasia, with an estimated incidence of 1:50,000 pregnancies [2]. Fewer than 100 cases have been documented in medical literature [3]. Although rare, clinical manifestations may include irregular vaginal bleeding, hemoptysis (in cases of pulmonary metastasis), or anemia and cachexia (with pelvic metastasis). However, some cases remain asymptomatic, particularly when no maternal-fetal metastasis has occurred, making prenatal diagnosis particularly challenging. Most IC cases are incidentally detected during routine placental histopathological examination.
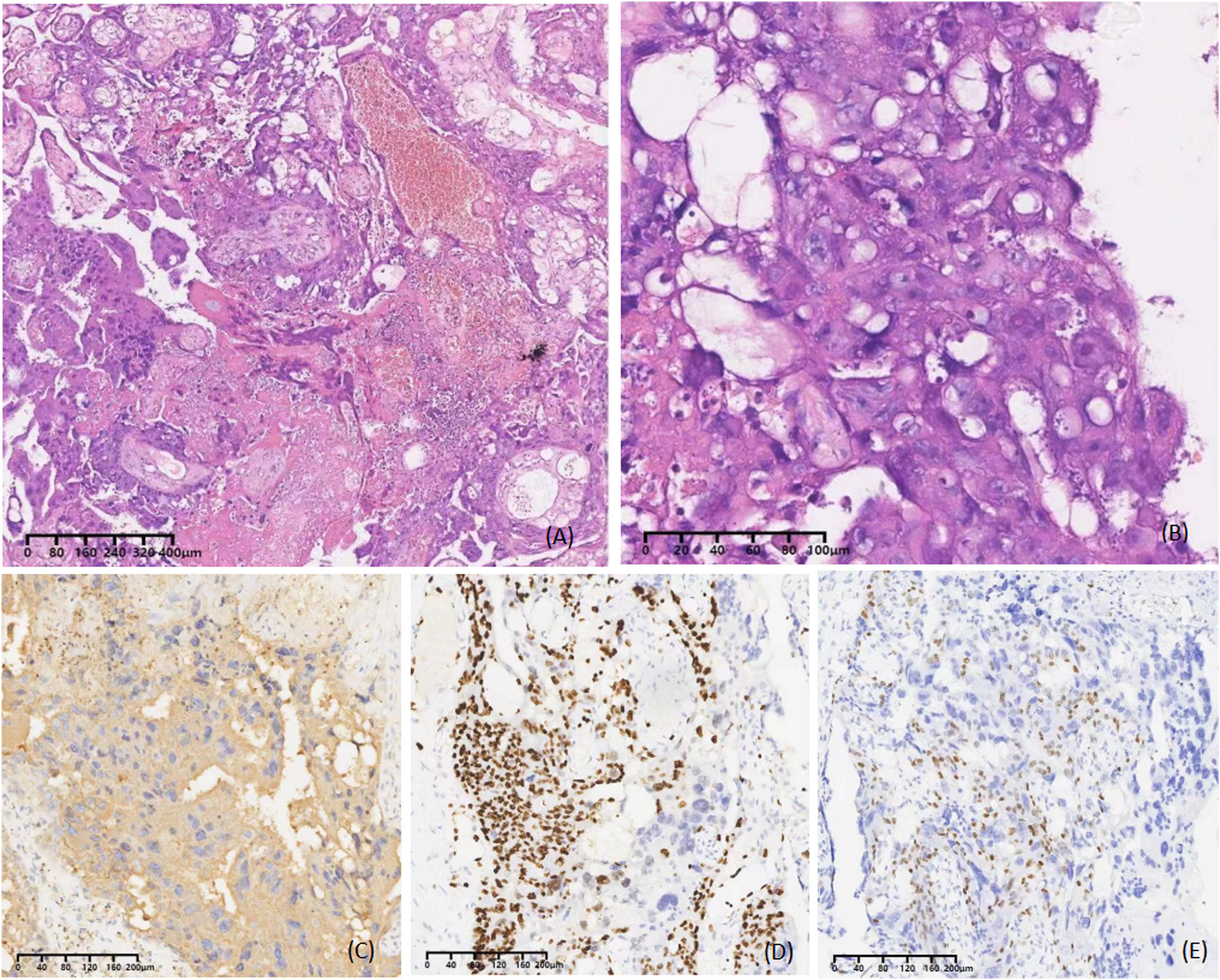
The patient in this case was in the third trimester and presented with intrauterine fetal distress. We promptly identified abnormal electronic fetal heart rate monitoring and performed an immediate emergency cesarean delivery, with no neonatal asphyxia occurring. Postpartum evaluation revealed fetal hemorrhage despite grossly normal placental morphology. Histopathological examination confirmed IC diagnosis, demonstrating characteristic microscopic findings including: (1) focal proliferation of cytotrophoblasts and syncytiotrophoblasts within villous spaces; (2) variable stromal and vascular invasion (distinct from conventional choriocarcinoma); (3) hemorrhagic necrosis of placental villi; and (4) intervillous space encirclement by abnormally proliferating trophoblasts. Immunohistochemical analysis showed positivity for p63, β-hCG, and Ki-67 in malignant trophoblastic cells.
IC may lead to significant obstetric complications including preterm delivery and intrauterine fetal distress, particularly during the third trimester. Although gross placental examination may appear normal, comprehensive histopathological evaluation remains essential to prevent diagnostic oversight. This case was successfully diagnosed due to the pathologist’s meticulous examination, considering the lesion measured only 12 × 7 × 3 mm in size. Notably, IC has been identified as an etiological factor in cases of unexplained massive fetomaternal hemorrhage [2, 4]. We recommend systematic postpartum placental histopathological assessment and serial β-hCG monitoring when such pregnancy complications occur.
There is currently no consensus on which patients should be screened for IC and on the appropriate management and surveillance. Since some patients with IC are asymptomatic, most involved pregnancies are uneventful and the placental lesion is usually small and can be easily missed, it is likely that many cases are missed and the true incidence may be higher than documented [2, 5, 6]. Although routine placental pathological examination may improve case detection rates, it concurrently elevates both healthcare expenditures and resource utilization. Therefore, we recommend: (1) directed placental examination for patients with pregnancy complications, and (2) systematic postpartum β-hCG surveillance for high-risk populations.
In terms of treatment, for non-metastatic intraplacental choriocarcinoma (IC), we recommend close monitoring of maternal serum β-hCG levels during the postpartum period, as these cases typically demonstrate favorable outcomes. In contrast, metastatic IC requires prompt initiation of chemotherapy, with treatment regimens following established protocols for gestational choriocarcinoma [7]. In comparison with other reported cases in the literature, the present case demonstrated no evidence of metastasis, with maternal serum β-hCG levels remaining within the normal range from the first postpartum month onward. Consequently, neither hysterectomy nor chemotherapy was required in this case.
Given that a substantial proportion of IC cases are asymptomatic and incidentally diagnosed, the true disease prevalence likely exceeds currently reported rates. To improve diagnostic detection, we advocate for thorough histopathological examination of the placenta in all clinically suspicious cases, including those with unexplained fetal distress or antepartum hemorrhage.
This case report highlights the importance of considering IC in the differential diagnosis of perinatal complications, particularly when evaluating cases with discordant clinical and pathological findings. Increased awareness of this entity may lead to earlier detection and appropriate management.