Study design and data source
This study employed a cross-sectional design to assess the prevalence and determinants of suicidal behaviours among adults living with cancer at Korle Bu Teaching Hospital in Ghana. The cross-sectional design was ideal for capturing a snapshot of suicidal ideation, attempts, and related factors at a single point in time. This design allowed for the exploration of associations between various factors (such as socio-demographic characteristics, mental health history, and support systems) and suicidal behaviours within this population.
Study site description
This research was conducted at Korle Bu Teaching Hospital (KBTH) in Accra, Ghana, the country’s largest tertiary healthcare facility and leading teaching hospital. KBTH serves as a national referral centre, drawing patients from across Ghana, including Greater Accra, Central, Eastern, Western, Volta, Ashanti, and parts of the Northern Region, as well as neighbouring countries such as Nigeria, Burkina Faso, and Togo [16]. It has 17 clinical and diagnostic departments/units, including three specialized centers and the first facility in Ghana to perform ureteroscopy.
Cancer care at KBTH is delivered through the National Centre for Radiotherapy, Oncology, and Nuclear Medicine, a major public oncology facility offering comprehensive cancer management services [17]. These include diagnostics, chemotherapy, external beam radiotherapy, brachytherapy (e.g., for prostate and cervical cancer), and palliative care. The Centre also serves as a training hub for medical students, oncology nurses, and other healthcare professionals [16, 17]. The oncology unit serves a socioeconomically diverse population comprising patients from both urban and peri-urban areas [16]. However, individuals from rural and remote regions may be underrepresented due to access and referral limitations. While the wide geographic reach of the centre enhances population diversity.
Study population
The study population consisted of all adult patients aged 18 years and older, diagnosed with cancer at Korle Bu Teaching Hospital.
Inclusion criteria
Adult patients (18 years or older) with a confirmed cancer diagnosis and the ability to understand and provide informed consent. All cancer types were eligible, including both solid tumors (e.g., breast, prostate, cervical, colorectal) and hematologic malignancies (e.g., leukemia, lymphoma). Also, patients currently receiving cancer treatment (chemotherapy, radiotherapy, hormonal therapy, or surgery) and those in follow-up care or palliative support were included.
Exclusion criteria
Patients with severe mental illness or terminal illness that affected their ability to participate in the study, as well as those who were unavailable during the data collection period, were excluded from the study. In addition, Patients with severe cognitive impairment, acute psychosis, active delirium, or any diagnosed neurodegenerative disorder that could compromise their ability to understand or respond to the questionnaire were excluded.
Sampling strategy
The study employed a convenience sampling method to recruit participants. Adults aged 18 years and above with a confirmed cancer diagnosis were selected from Korle Bu Teaching Hospital in Accra, Ghana. Participants were approached during their routine visits across oncology, radiotherapy, and surgical units to ensure a diverse representation of cancer types and treatment stages. Those who met the eligibility criteria and were available and willing to provide informed consent were enrolled.
This method was chosen due to practical constraints, including time limitations, lack of access to a comprehensive cancer registry, and resource limitations, which made random sampling infeasible. Convenience sampling allowed for efficient recruitment within the hospital setting and ensured the inclusion of patients actively engaged in care.
However, this non-random approach introduces potential selection bias, as individuals who were more readily available or willing to participate may differ systematically from those who were not. As a result, the findings may not be fully generalizable to all cancer patients in Ghana. Future studies employing probability sampling methods are recommended to improve representativeness and external validity.
Sample size determination
The sample size for the study was calculated using Cochran’s (1977) formula, which is widely employed to estimate sample sizes for surveys. The formula applied is: (:n=frac{{z}^{2}times:p(1-p)}{{d}^{2}})
Where:
n = Sample size.
Z = The z-score that corresponds with a 95% confidence level, typically 1.96.
P = Estimated prevalence of malaria (set at 50% due to the lack of available data).
d = Margin of error set at 5% (0.05)
$$eqalign{n & =frac{{1.96}^{2}times:0.5times:(1-0.5)}{0.05times:0.05} cr & =384cr & 384}$$
To address potential non-response and incomplete data, we increased the minimum sample size by 10%, resulting in a final sample size of 405 adult cancer patients. This adjustment ensured that the sample would remain adequate despite any potential dropouts or missing data, thus enhancing the reliability of the study’s findings.
Data collection methods and instruments
The study used structured, self-administered questionnaires to collect data on suicidal behaviours among adults living with cancer at Korle Bu Teaching Hospital. A standardized assessment tool, the Columbia-Suicide Severity Rating Scale (C-SSRS), was employed to evaluate the severity of suicidal ideation, attempts, and behaviours. In addition to the C-SSRS, a structured questionnaire was used to gather information on various factors influencing suicidal behaviour, such as socio-demographic variables, mental health history, life stressors, support systems, and experiences of abuse. The questionnaire was adapted from existing literature and modified to align with the study’s objectives.
It was structured into four components, with the first section assessing socio-demographic characteristics like age, sex, and educational background, and the second and third sections focused on the study’s main objectives. Trained research assistants administered the tools to eligible participants, ensuring they understood each question and responded appropriately. A week’s training session was held for the interviewers, equipping them with a thorough understanding of the questionnaire and ethical considerations, ensuring adherence to protocols throughout the data collection process. This approach allowed for a comprehensive assessment of suicidal behaviours and their influencing factors, while maintaining confidentiality and participant comfort. It took an average of 10 to 15 min to administer the full questionnaire, and Data collection lasted for two months.
Ethics approval and consent to participate
Ethical approval for the study was obtained from the University of Health and Allied Sciences Review Ethics Committee (UHAS-REC A.30 [111]22–23) and the Institutional Review Board of the Korle Bu Teaching Hospital’s Research Department. Informed consent was obtained from all participants after they were fully briefed about the study’s purpose, procedures, risks, and potential benefits. Given the sensitive nature of the topic, the study acknowledged the potential risk of triggering mental health issues, such as distress or emotional discomfort, during data collection. To address these risks, the following measures were implemented: participants were informed of their right to withdraw from the study at any point without consequence; they were provided with a list of mental health support services, including counsellors and helplines, should they feel distressed; trained research assistants were available to provide immediate support or assistance if needed; and any participant showing signs of distress was immediately offered a referral for counselling. Confidentiality was ensured through the use of pseudonyms, and all data was securely stored in an encrypted, password-protected database, with access limited to the Principal Investigator and the research supervisor. The study adhered to strict ethical guidelines to protect the rights and well-being of all participants.
Study variables
Dependent variable
The outcome variables of suicidal ideation, suicidal behaviour, suicidal plan, and suicidal attempt were measured using the Columbia-Suicide Severity Rating Scale (C-SSRS).
Prevalence variable
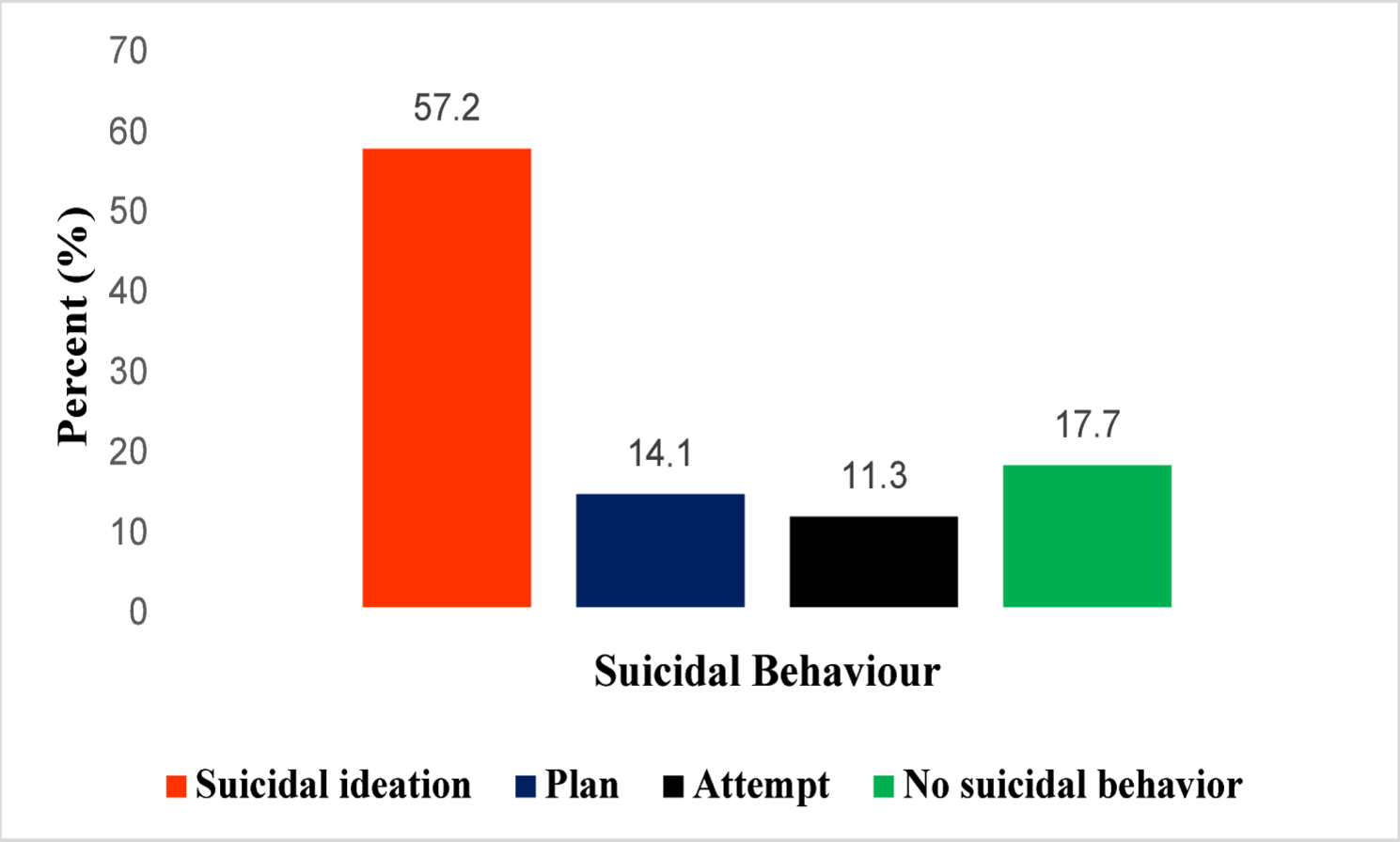
In this study, suicidal behaviour was measured using the Columbia-Suicide Severity Rating Scale (C-SSRS), which evaluates suicidal ideation, plans, attempts, and behaviours.
Definition and coding of suicidal behaviour outcomes
Suicidal behaviours were assessed using the Columbia-Suicide Severity Rating Scale (C-SSRS), which evaluates suicidal ideation, suicidal planning, and suicidal attempts. In this study, three primary binary outcomes were generated:
-
Suicidal ideation was coded as 1 (Yes) if the participant endorsed either passive or active thoughts of killing themselves and 0 (No) if not. This included any level of ideation severity as per the C-SSRS screener [17, 18].
-
Suicidal plan was coded as 1 (Yes) if the participant indicated they had formulated a method, timing, or intent to carry out suicide, and 0 (No) if otherwise.
-
Suicidal attempt was coded as 1 (Yes) if the participant reported any self-injurious behaviour undertaken with at least some intent to die, regardless of whether actual harm occurred. This also included aborted or interrupted attempts. Those with no such behaviours were coded as 0 (No).
Participants who answered “No” to both ideation screening questions were skipped to the behaviour section. For those who answered “Yes,” additional probing followed, including questions on ideation intensity (frequency, duration, controllability, and deterrents). Ideation duration was categorized as fleeting, < 1 h, 1–4 h, 4–8 h, or persistent (> 8 h). Participants were also asked whether deterrents (e.g., family obligations, religious beliefs) had prevented action [17, 18].
For descriptive purposes, a composite suicidal behaviour variable was also derived. This variable was coded as 1 (“Yes”) if a participant endorsed any of the three outcomes—ideation, planning, or attempt, and 0 (“No”) if none were reported. This allowed for the estimation of overall suicidal behaviour prevalence, consistent with standard epidemiological reporting in mental health research [17]. While the C-SSRS allows for risk classification into low (ideation only), moderate (ideation plus vague planning), and high (planning with intent or attempt), these categories were not used in inferential statistical modelling [18]. All suicidal behaviour variables were treated as separate binary outcomes for logistic regression analysis. This coding strategy ensured consistency with C-SSRS thresholds and enabled both outcome-specific and composite-level analyses of suicidal behaviours among cancer patients.
Independent variable
The explanatory variables in this study included socio-demographic factors (such as age, gender, marital status, and education level), mental health diagnoses (depression and anxiety), experiences of abuse (physical and emotional), and feelings of helplessness or being a burden. Other factors considered were the presence of a support system, recent significant life changes after diagnosis, and the perception of hopelessness or lack of solutions to personal problems. These variables were assessed to determine their influence on suicidal ideation and behaviour among adults living with cancer. The study aimed to identify key risk factors for suicidal behaviours that could inform preventive interventions.
Statistical analysis
Data collected through structured questionnaires and the Columbia-Suicide Severity Rating Scale (C-SSRS) were entered into Stata version 17 for analysis. Descriptive statistics, including frequencies, percentages, and means, were used to summarize sociodemographic characteristics and the distribution of suicidal behaviours. Bivariate analyses (Chi-square tests for categorical variables and t-tests for continuous variables) were conducted to explore associations between suicidal outcomes and potential predictors, including sociodemographic variables, psychosocial stressors, mental health history, and social support. Three separate binary logistic regression models were fitted for each suicidal behaviour outcome: ideation, planning, and attempt, each coded as a dichotomous variable (Yes = 1, No = 0) based on participant responses to the C-SSRS. The C-SSRS cut-offs used were: endorsement of passive or active suicidal thoughts (ideation), formulation of a method or intent (plan), and any self-reported non-fatal suicidal behaviour (attempt), in line with standard scoring guidelines.
Variables with a p-value < 0.20 in the bivariate analyses, along with theoretically relevant covariates, were included in the multivariable models. To ensure no serious multicollinearity, Variance Inflation Factors (VIFs) and Tolerance values were calculated separately for sociodemographic predictors and psychosocial factors (see Tables 6 and 8). All variables included in the final models had VIFs below 2.0, indicating acceptable independence among predictors. Model fit was evaluated using the Hosmer-Lemeshow goodness-of-fit test and Nagelkerke’s R² to assess the explained variance (see Table 9). Missing data were minimal (less than 5% per variable). After examining patterns of missingness, we applied a complete case analysis approach. No data imputation was performed.
Adjusted odds ratios (aORs), 95% confidence intervals (CIs), and p-values were reported for each predictor in the final regression models. The 95% CIs were computed using the standard error of the regression coefficient (β), assuming asymptotic normality, with the formula: exp(β ± 1.96 × SE). This interval estimates the range within which the true odds ratio is likely to fall with 95% certainty. A 95% CI that does not include 1.0 indicates a statistically significant association. For instance, an aOR of 3.0 with a 95% CI of 1.5–5.2 suggests that individuals with that exposure are three times more likely to exhibit the suicidal outcome, and the association is considered statistically significant because the confidence interval does not cross the null value (1.0).