22/10/2025
2264 views
31 likes
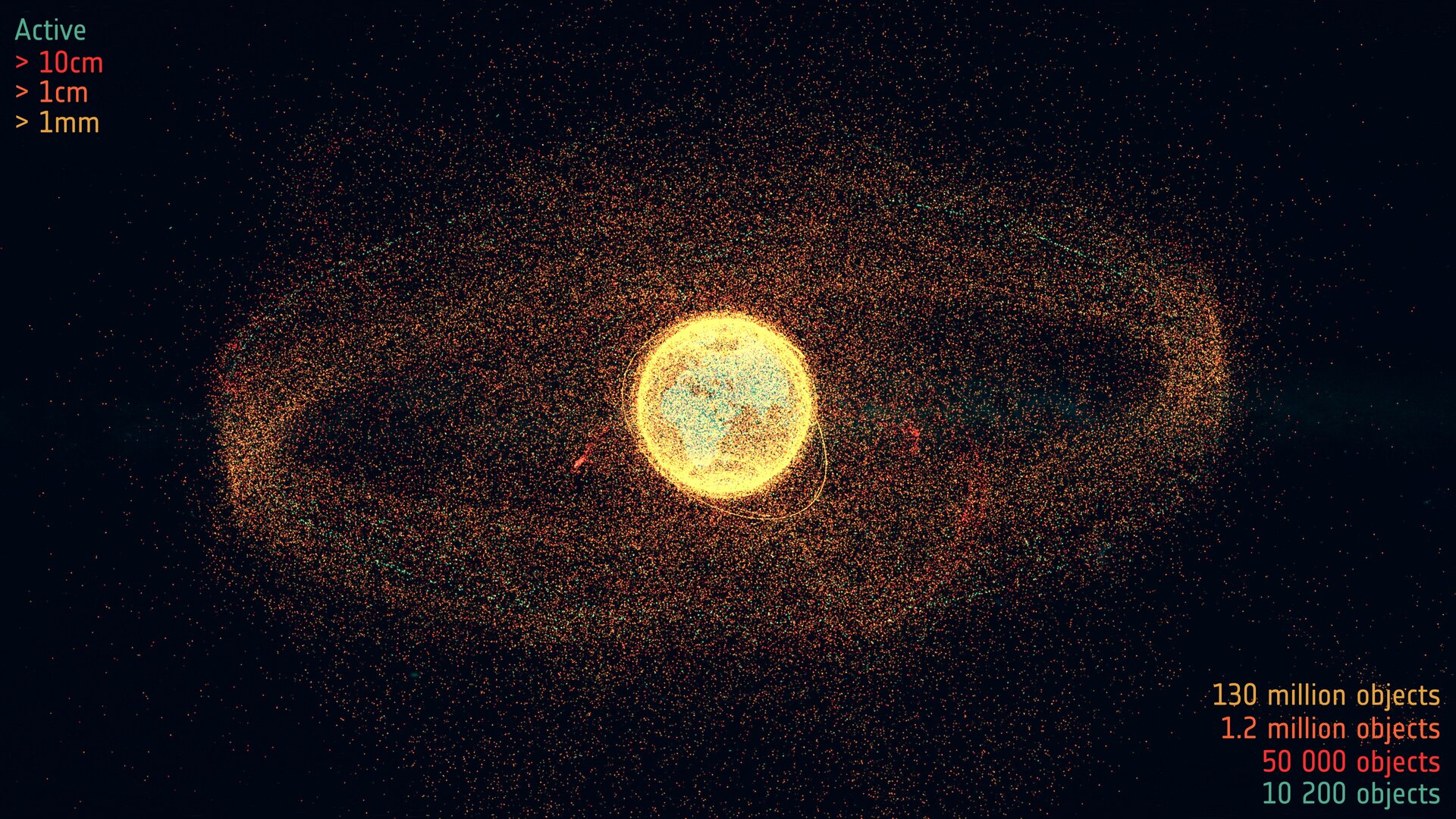
The congestion and pollution of Earth orbit is quickly getting worse. We need to be able to quantify how our behaviour impacts the orbital environment in…
22/10/2025
2264 views
31 likes
The congestion and pollution of Earth orbit is quickly getting worse. We need to be able to quantify how our behaviour impacts the orbital environment in…