 Getty Images
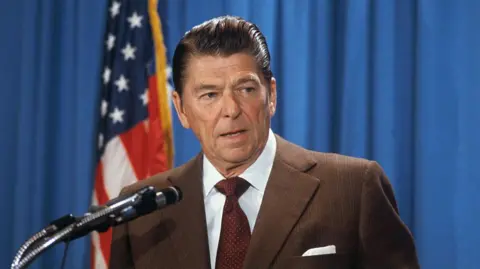
Getty ImagesUS President Donald Trump halted all trade negotiations with Canada earlier this week over an advert in which former President Ronald Reagan says…
 Getty Images
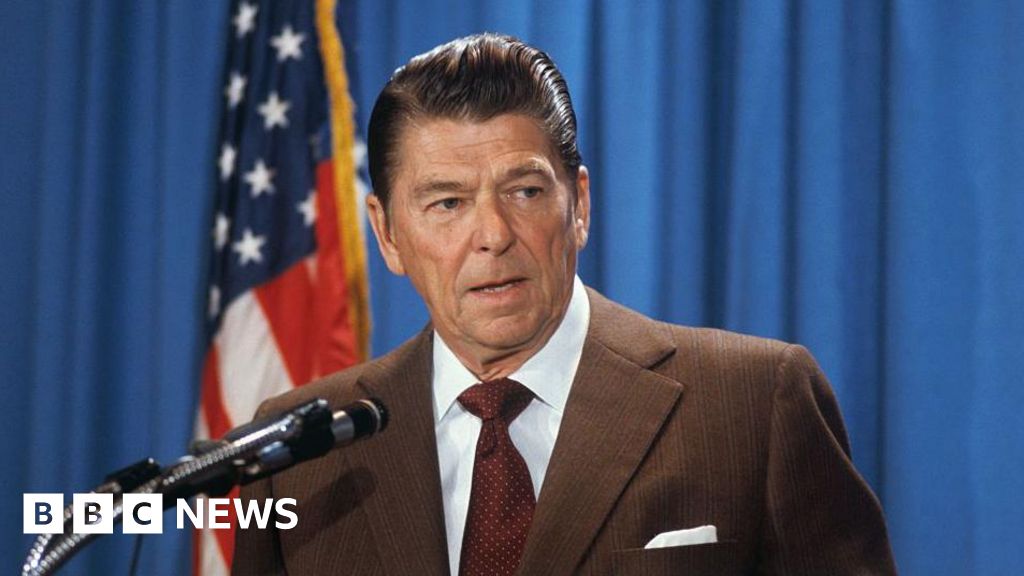
Getty ImagesUS President Donald Trump halted all trade negotiations with Canada earlier this week over an advert in which former President Ronald Reagan says…