
A 33-year-old male presented to the Emergency Department with unilateral painless loss of vision of 1.5 hours duration. He had a past medical history of T4N0M0 follicular thyroid cancer in remission for several years post total thyroidectomy and radioactive iodine, as well as myopia post LASIK surgery. The patient described the loss of vision in his left eye as sudden onset and atraumatic, occurring while he had been walking, accompanied by transient giddiness and tinnitus. There were no concurrent symptoms of floaters, flashes, headaches, or scalp tenderness.
On examination, the left eye exhibited markedly reduced visual fields, sparing only a small island on the temporal side, through which the visual acuity scoring was 6/6 on Snellen chart testing. The right eye was unaffected. There were no foreign bodies, the conjunctiva was not injected, and the extraocular movements were full and intact. The direct pupillary reflexes were intact; however, a left relative afferent pupillary defect was noted. Slit lamp examination showed that the anterior chamber was deep and quiet, and the lens was clear. The left optic disc was noted to be pale with the cilioretinal artery area spared on fundoscopy (Fig. 1). Intraocular pressure was normal at 16mmHg on the left, and 13mmHg on the right. The rest of the neurological examination was unremarkable except for an inconsistent, patchy reduction of sensation over cranial nerve V1-2 distribution. Systemic examination did not reveal any carotid bruit, murmur, organomegaly, or bleeding diasthesis. The patient was normotensive and a random capillary blood glucose was 6.1 mmol/L.
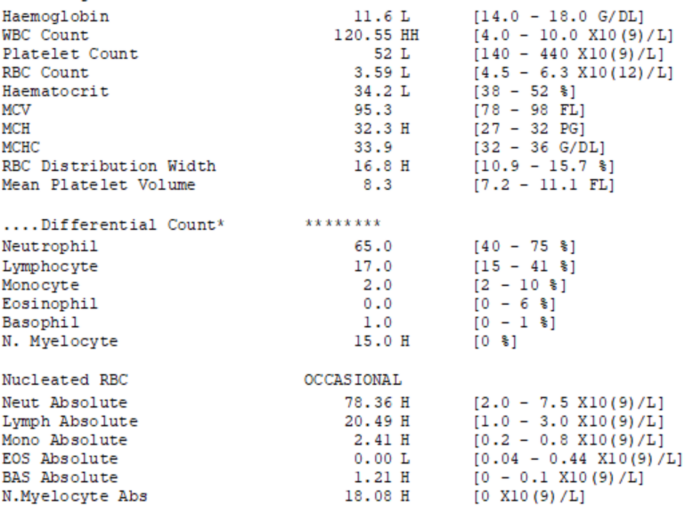
The patient’s electrocardiogram was of a normal rhythm. Initial blood tests elucidated a leukocytosis with a white blood cell count of 120.55 × 109/L, predominantly myelocytes and neutrophils with occasional cells showing a high nuclear to cytoplasm ratio. No promyelocytes were noted and there was bicytopenia of the other two cell lines (Fig. 2).
The patient was urgently referred to the ophthalmologist and haematologist. Anterior chamber paracentesis was performed and the patient was initiated on brimonidine eye drops. He began treatment with leucopheresis, hydroxyurea, allopurinol, and aggressive IV hydration. Further investigations included Magnetic Resonance Imaging (MRI) with contrast of the brain which showed mild diffusion restriction noted in the nasal retina of the left globe and within the left retrobulbar optic nerve (Fig. 3) consistent with ischaemic changes. Some degree of flow attenuation was noted in the left ophthalmic artery as compared to its counterpart on the right side (Fig. 4). There was no aneurysmal vessel, large vessel occlusion, nor flow limiting stenosis seen.
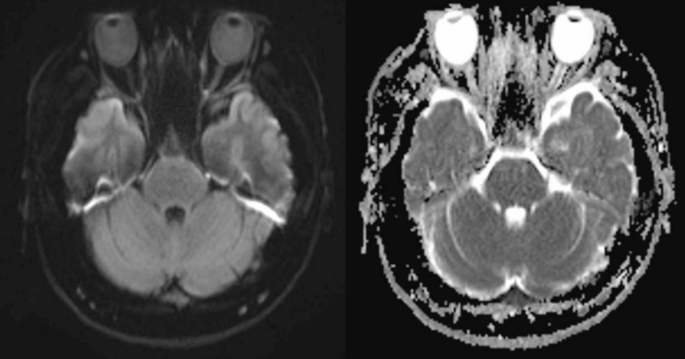
MRI Brain DWI sequence showing showed mild diffusion restriction in the nasal retina of the left globe and within the left retrobulbar optic nerve
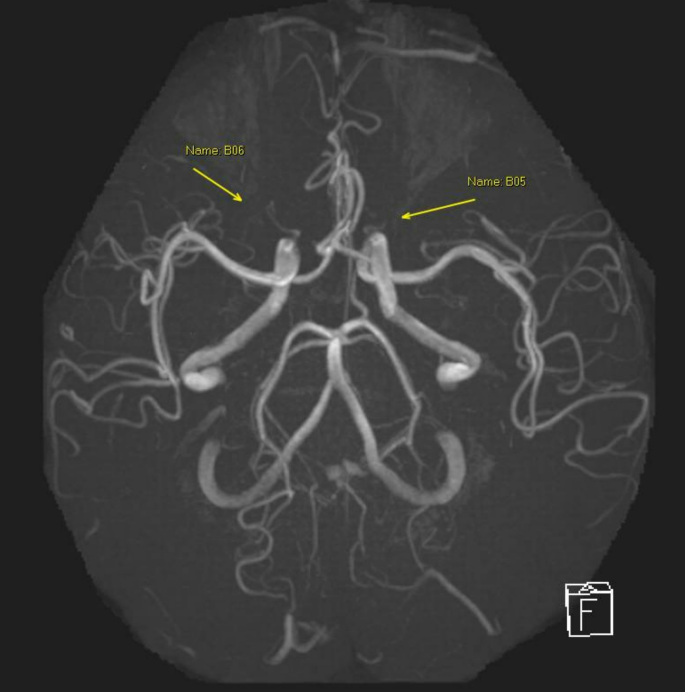
MRA ophthalmic artery showing flow attenuation in the left ophthalmic artery as compared to the right
A bone marrow aspiration was performed which showed marked myeloid hyperplasia with dysgranulopoiesis, mildly reduced megakaryopoiesis, and 22% blasts consistent with myelodysplastic or myeloproliferative neoplasms in high grade transformation to acute leukaemia, likely myeloid lineage. The flow cytometry showed 20% blasts with markers consistent with early T cell precursor acute lymphoblastic leukaemia. The trephine revealed a hypercellular marrow with marked increase in myelopoiesis and abnormal aggregates of immature myeloid/blast cells, as well as decreased erythropoiesis and megakaryopoiesis. The overall histological findings suggested a possible myeloproliferative neoplasm with transformation to acute leukemia. The final diagnosis of left eye CRAO secondary to hyperviscosity from leukocytosis due to T lymphoid and myeloid mixed phenotype acute leukaemia (MPAL) was confirmed.
The haematologist initiated treatment with fludarabine, cytarabine, granulocyte colony stimulating factor, idarubicin (FLAG-Ida) with close monitoring. During his inpatient stay the patient developed bleeding from vascular access and bone marrow aspirate sites, requiring fresh frozen plasma, cryoprecipitate, and fibrinogen concentrate transfusions. On follow-up, the patient reported slight improvement to his visual fields with some recovery of the central vision.