PBD is a unique histological type of BD. The etiology and pathogenesis of BD (including PBD) have not yet been fully elucidated. Possible pathogenic factors include arsenic exposure, human papillomavirus infection, skin damage (insect bites, trauma, heat injury, etc.), inflammatory skin diseases, genetic factors [8,9,10,11,12,13]. The clinical manifestations of BD include single or multiple slow-growing erythematous lesions with clear boundaries, mild bulges, irregular shapes, and diameters ranging from a few millimeters to a few centimeters. Skin lesions can exhibit pigmentation, verrucous hyperplasia, hyperkeratosis or crusting [2]. Lesions can occur on the skin or mucous membranes of any part of the body, often on the head, trunk, and limbs, and rarely on the palms, soles, nail beds, nipples, or areolas [3,4,5]. Currently, there are only 11 reported cases of BD occurring in the nipple-areola complex, 3 cases of PBD occurring in the nipple-areola complex, and 1 case of PBD occurring in the nipple region documented in the literature [5, 6, 14, 15]. Interestingly, all the above patients were female patients. In the present case, the patient was an older person, and the nipple was the site of occurrence. To the best of our knowledge, this is a rare report of PBD occurring in the male nipple area, which is rare and increases the difficulty of diagnosis. The patient was treated for eczema for a long time, and no obvious improvement was observed. In this case, the five male sex hormone levels and HPV DNA detection were normal. It is worth further exploring the sex differences in the incidence of PBD in the nipple or nipple-areolar complex.
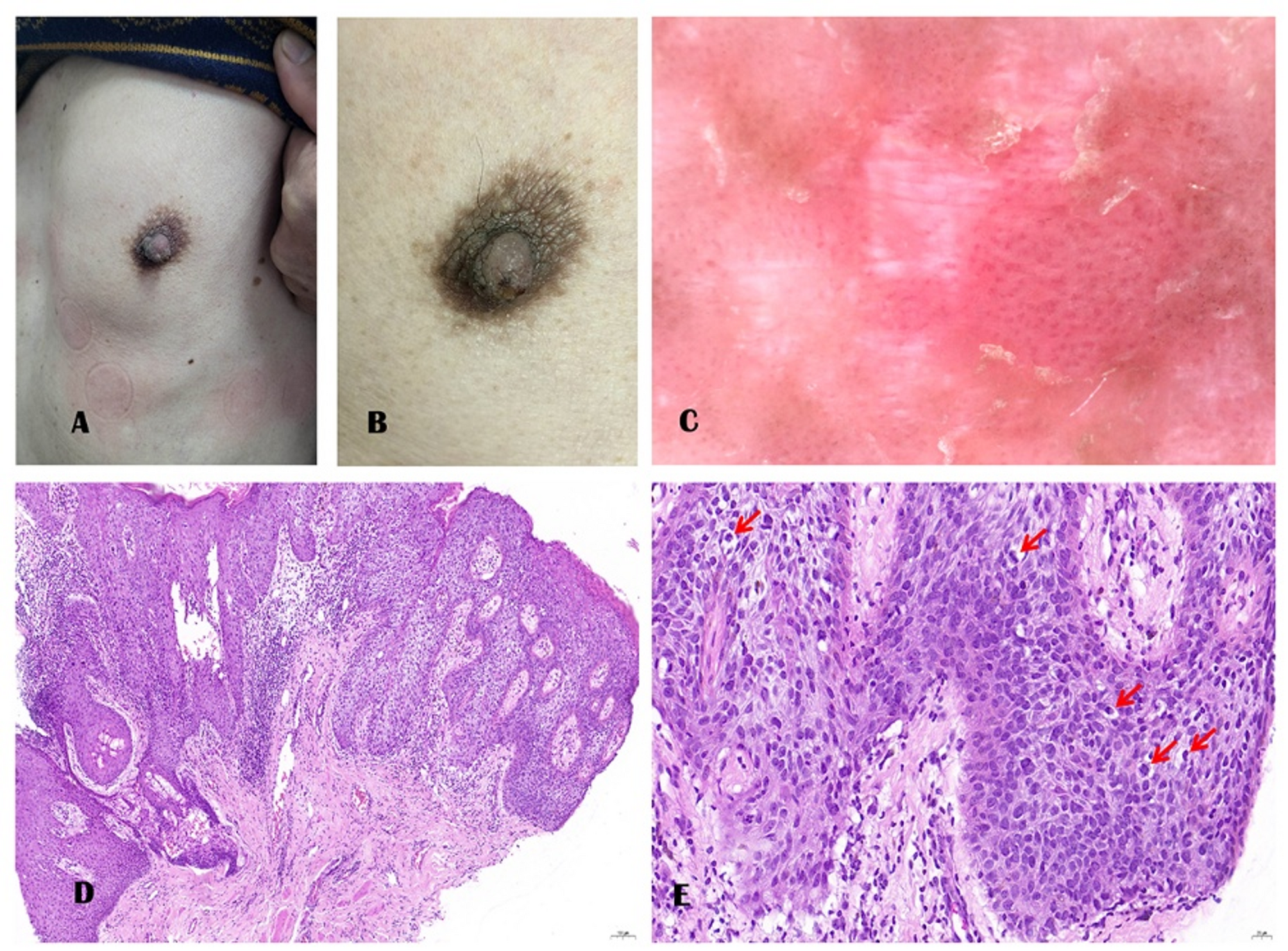
BD (including PBD) dermoscopy can provides diagnostic clues. Glomerular blood vessels and surface scales can be observed on a clear reddish-brown background. Dermoscopy is convenient and noninvasive, and can be used to identify early lesions and improve the accuracy of diagnosis [9, 16]. Histopathological examination remains the gold standard for diagnosis. Pathological examination showed that the entire epidermis was dysplastic, involving the entire epidermis including skin appendages. It is often accompanied by incomplete keratinization, acanthosis, complete disorder of the epidermal structure, loss of cell polarity, common nuclear division, and an intact basement membrane. It must be differentiated from diseases such as MPD, EMPD, superficial disseminated melanoma, eczema, and psoriasis.
Significant morphological and immunophenotypic overlaps may exist between PBD and MPD [17]. In the past, it was believed that Pagetoid cells in MPD were positive for CEA and low-molecular-weight keratins CK5/6, CK7, and CK8, whereas those in BD (including PBD) were negative for CEA and low-molecular-weight keratins, which could be used as specific indicators to distinguish between the two diseases [18]. However, recent studies have reported that CEA and CK7 are also expressed in PBD, increasing the difficulty of identification [18,19,20,21,22]. PAS and GCDFP-15 are usually positive in Paget’s disease but negative in PBD [23]. Approximately one-third of Paget’s disease cases are HER-positive, and PBD is HER-negative [24, 25]. In addition, Melan A, HMB45, and S-100 can be used to differentiate between PBD and superficial disseminated melanoma [26]. Raju considered PAS staining a sensitive indicator for identifying PBD and other diseases with Pagetoid cells in the epidermis, such as hypertrophic actinic keratosis, superficial disseminated melanoma, MPD, and EMPD [18, 27, 28]. P40 and P63 are typically negative in MPD and EMPD, which helps to differentiate Paget’s disease from squamous cell lesions, such as PBD. In this case, CK7, CEA, S-100, HMB-45, GCDFP-15, HER, CAM5.2, and PAS were negative, CK 5/6,P40,P63 were diffuse positive in neoplastic cells, supporting the diagnosis of PBD rather than MPD or superficial disseminated melanoma. Table 1 summarizes the different immunohistochemical expression levels in PBD, MPD, EMPD, and superficial disseminated melanoma.
It is worth pondering that the skin lesions on the left nipple of this patient resembled eczema, and no significant improvement was seen after long-term treatment for eczema. MPD are often associated with breast cancer and usually originate in the mammary ducts. Therefore, MPD clinical lesions usually start at the nipple and extend to the nipple and surrounding skin [29]. The patient presented with skin lesions solely affecting the nipple, strongly suggesting the possibility of MPD. Histopathological examination of the patient’s tissue revealed widespread Pagetoid cells that were visible throughout all layers and exhibited marked pleomorphism. Unlike MPD, where Pagetoid cells are more commonly found in the middle and lower layers of the epidermis and exhibit a scattered or nest-like distribution with less pronounced pleomorphism, the likelihood of MPD remains higher than that of PBD. Without the aid of immunohistochemistry, it is challenging to differentiate between PBD and MPD based on existing diagnostic clues. Given that different diseases require different subsequent treatments, surgical excision ranges, and follow-up periods, accurate diagnosis is crucial.
Owing to the potential for invasive growth of BD (including PBD) skin lesions, early diagnosis and timely treatment are crucial. Surgical excision is recommended if the lesion is small. Mohs micrographic surgery can maximize aesthetic improvement and reduce functional defects. General lesions can be treated with cryotherapy, electrocautery, laser and photodynamic therapy, or radiotherapy. In this case, the patient was an older person with low aesthetic requirements. Therefore, radical resection of the skin tumor on the left breast was performed, and the patient recovered well postoperatively.