Study settings and study population
In 2019, to understand the disease burden of chlamydia infection among reproductive-aged women (18–44 years) and further develop chlamydia screening strategies, the Guangdong Provincial Center for Skin and STIs Control conducted a cross-sectional survey in Guangdong province, which has been described previously [18]. This is a secondary data analysis of the study. In short, study settings were determined by stratified sampling. Twenty-one cities of Guangdong Province were stratified into three groups (high, medium, and low) using tertiles of the reported chlamydia incidence rates in 2017. Specifically, the 21 cities were ranked in descending order of incidence, with the top 7 cities (highest tertile) classified as ‘high’, the middle 7 as ‘medium’, and the bottom 7 (lowest tertile) as ‘low’. Data were obtained from the China Information System for Disease Control and Prevention. Within each tertile, one or two hospitals were randomly selected for inclusion. Finally, Dongguan Houjie Hospital in Dongguan (high), Yunfu People’s Hospital and Xinxing No.1 People’s Hospital in Yunfu (medium), and Zhanjiang Women and Children’s Hospital in Zhanjiang (low) were chosen to be included to conduct the survey.
This study included women who were 18 to 44 years old, sought health care in the gynecological department for the first time in the last 12 months, had ever had sex with men, and were willing to receive a chlamydia test. Those who had a vaginal administration within 24 h were excluded. Information about baseline characteristics was collected through online questionnaires (Wenjuanxing platform), including sociodemographic characteristics, medical history, sexual behaviors, and the use of antibiotics in the past 12 months (by self-report with nurse assistance): azithromycin, erythromycin, benzylpenicillin, amoxicillin, ceftriaxone, clindamycin, and metronidazole. This questionnaire has been used in our previous study [18].
The study was approved by the Institutional Review Board of the Dermatology Hospital of Southern Medical University (GDDHLS-20181207). All participants provided written informed consent.
Sample collection and laboratory testing
Women were tested for chlamydia and gonorrhea by self-collected first-stream urine and/or nurse-taken cervical swabs during the visit. All samples were stored under 2 to 8℃, and testing was done by nucleic acid amplification test (NAAT) (Cobas® 48000 CT/NG Amplification/Detection Kit, Shanghai, China) in the Dermatology Hospital of Southern Medical University.
Definitions
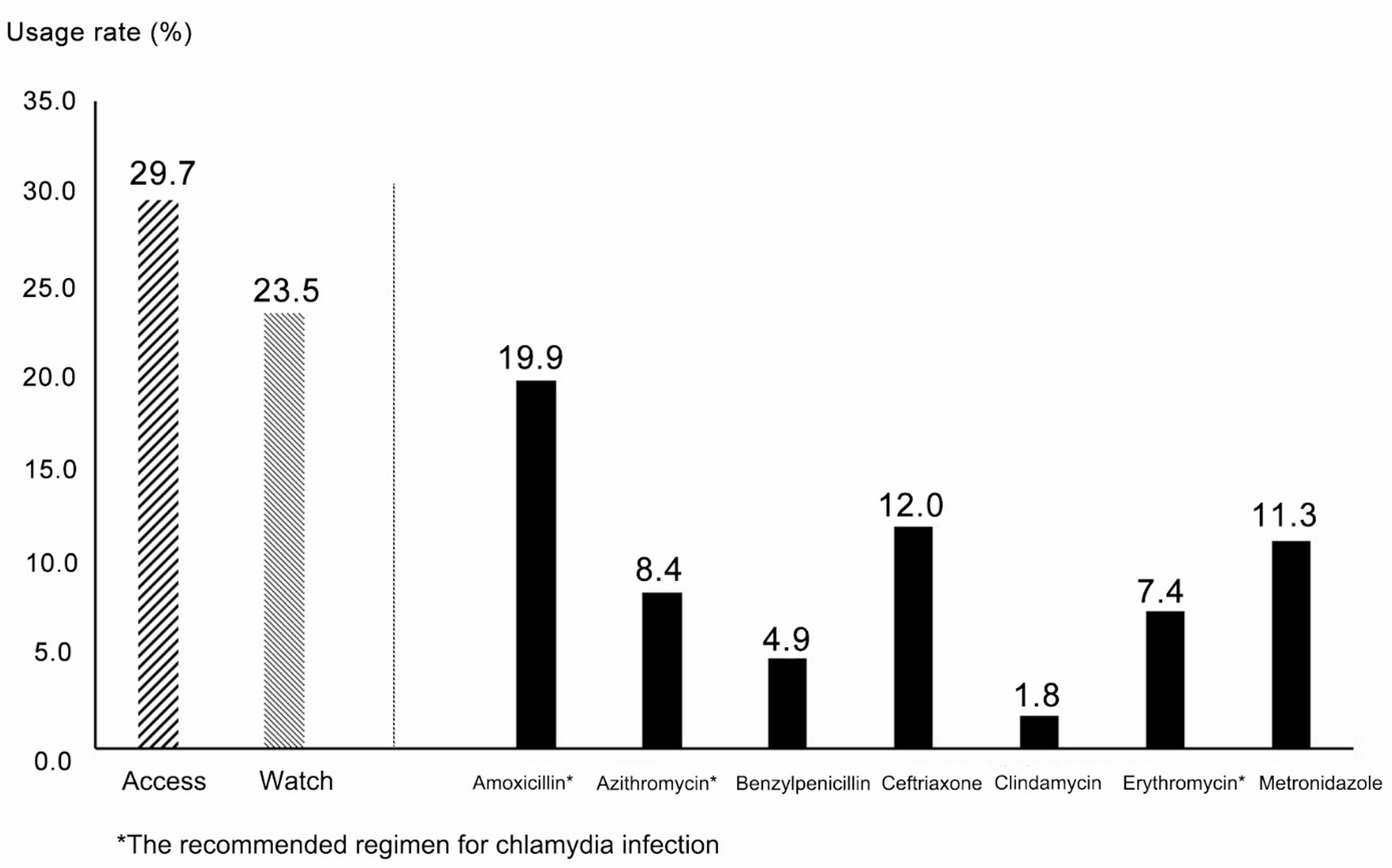
Antibiotic use refers to using at least one of the seven antibiotics (azithromycin, erythromycin, benzylpenicillin, amoxicillin, ceftriaxone, clindamycin, and metronidazole) preceding the visit within 12 months. Participants were asked about each antibiotic with three response options: “yes,” “no,” or “unsure.” Only explicit “yes” responses were classified as antibiotic use. These seven antibiotics were chosen because of their extensive use in gynecological department settings. Azithromycin, amoxicillin, and/or erythromycin use is the recommended regimen for chlamydia infection according to the Guidelines for the Clinical Diagnosis, Treatment and Prevention of Sexually Transmitted Diseases. Azithromycin is the recommended regimen for chlamydia infection, and erythromycin is an alternative regimen among adolescents and adults. Amoxicillin is an alternative regimen for pregnant women [5]. We further classified the antibiotics into different categories based on the WHO AWaRe system -Access (Amoxicillin, Clindamycin, Benzylpenicillin, Metronidazole), recommended as empiric first or second-choice treatment options for common infections, and Watch (Azithromycin, Ceftriaxone, Erythromycin) (Reserve antibiotics were not applicable in this study) [19].
Current chlamydia and gonorrhea infections were based on positive urine and/or cervical swab results. Ever having a casual sex partner and/or not constantly using condoms during sex were regarded as having high-risk sexual behaviors.
Statistical analysis
Baseline characteristics were compared between women with and without antibiotic use using Pearson’s χ² test for categorical variables (presented as counts and percentages). Missing data on baseline characteristics were grouped in a separate category per variable. The proportion of different antibiotic use was calculated. Association between prior antibiotic use and the prevalence of chlamydia infection was assessed by multivariable logistic regression, calculating odds ratios (ORs) with their corresponding 95% confidence intervals (CIs), adjusting for age, age at first sexual debut, and high-risk sexual behaviors. For antibiotics specifically recommended for chlamydia treatment (azithromycin, erythromycin, amoxicillin), we conducted a subgroup analysis among users of these agents to assess class-specific effects.
All analyses were performed using R software (version 4.3.2; R Core Team, 2023). Statistical significance was considered at a two-sided P value < 0.05.