This retrospective cohort study included data from consecutive PAS cases diagnosed and managed at the University of Maryland Medical Center between May 2015 and December 2024. The study was approved by the University of Maryland Institutional Review Board (HP-00079290). Patients who required delivery due to preeclampsia with severe features, abnormal fetal Doppler findings, or preterm premature rupture of membranes (PPROM) were excluded.
Standardized algorithm
A standardized algorithm was applied to determine the timing of delivery in PAS cases, based on both the number of antepartum bleeding episodes and the last cervical length measurement. PAS was diagnosed using transabdominal and/or transvaginal ultrasound (Voluson E8/E10, GE Healthcare, Milwaukee, WI, USA) and/or magnetic resonance imaging (MRI).
Cervical length was measured transvaginally by trained sonographers [18]. In PAS cases, cervical length was routinely measured after 30 weeks of gestation to assess preterm delivery risk and assist with delivery planning. For patients followed at our center, weekly serial measurements were performed. For late referrals, at least one measurement was obtained prior to delivery.
Antepartum bleeding was described as bright red vaginal bleeding more than spotting (approximately 10–20 mL) that started after 20 weeks of gestation without significant cervical shortening in transvaginal or transperineal ultrasound. Patients were admitted for observation immediately upon presentation, and if bleeding resolved, they were monitored for an additional 5–7 days. Patients were discharged if no recurrence occurred during this period. A new bleeding episode was recorded if vaginal bleeding reappeared at least 7 days after resolution of a previous episode. The number of antepartum bleeding episodes was categorized as none (0), one (1), or two or more (≥ 2).
Urgent delivery due to bleeding was indicated when the bleeding was either severe (> 500 mL within a few hours) or slow but persistent for over 24 h, in conjunction with maternal hemodynamic instability (hypotension, tachycardia), or non-reassuring fetal heart rate tracing. Urgent delivery was defined as delivery occurring before the scheduled time due to spontaneous vaginal bleeding or preterm contractions unresponsive to medical management, requiring immediate intervention by the obstetric team. Elective delivery was defined as delivery performed at the planned gestational age according to the standardized algorithm.
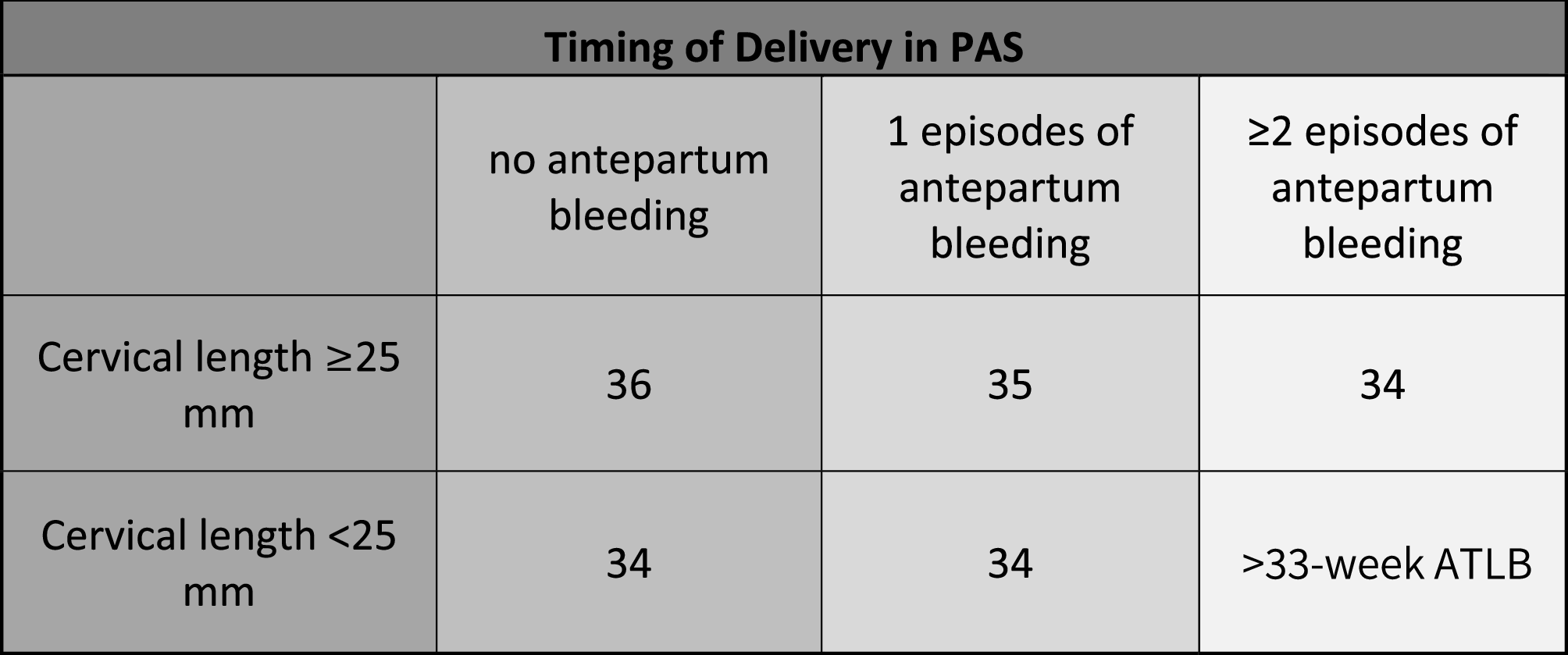
For patients with a cervical length of ≥ 25 mm, delivery was planned at 36 weeks in the absence of antepartum bleeding. If a patient experienced one episode of antepartum bleeding, delivery was scheduled at 35 weeks, whereas those with two or more episodes were delivered at 34 weeks.
For patients with a cervical length of < 25 mm, delivery was planned at 34 weeks in the absence of antepartum bleeding. If a patient experienced one episode of bleeding, delivery was scheduled at 34 weeks, whereas those with two or more episodes were delivered at the time of the last bleeding episode, provided it occurred beyond 33 weeks of gestation (Fig. 1). The timing of delivery was decided in a multidisciplinary meeting using the described standardized algorithm. The timing was discussed with the patient, and agreement was obtained.
Algorithm for timing of delivery in placenta accreta spectrum. ATLB: At the time of the last bleeding episode, PAS: placenta accreta spectrum
All patients were planned to receive a standard course of antenatal corticosteroids for fetal lung maturation, administered in two doses 24 h apart. If delivery could not be delayed beyond 24 h after the first dose, the second dose was omitted. Corticosteroids were administered after 34 weeks if not previously given [19]. Surgical management included cesarean hysterectomy or cesarean section with focal resection, depending on the extent of placental invasion and intraoperative findings. PAS diagnosis was confirmed intraoperatively based on surgical findings, and histopathological examination was performed when hysterectomy or focal resection was conducted. Intraoperative diagnosis of PAS was based on visual evidence of abnormal placental adherence to the uterine wall, difficulty with placental separation, or profuse hemorrhage from the placental bed [20]. Histopathologic confirmation, when available, was based on the presence of chorionic villi directly attached to or invading the myometrium.
Data collection
Demographic, clinical, and perinatal data were prospectively documented by obstetric care providers in the hospital records and obstetric database (Viewpoint 5.6, GE, PA, USA) during routine clinical care and retrospectively extracted for this study. Variables included maternal age, body mass index (BMI, kg/m²), parity, number of prior cesarean sections, history of preterm birth, placenta previa, gestational age (GA) at the last cervical length measurement, last cervical length, GA at delivery, type of surgery (cesarean section with focal resection, cesarean hysterectomy), estimated blood loss, number of packed red blood cells (pRBC), more than 4 units of pRBCs, admission to the intensive care unit (ICU), cystotomy, ureteral injury, number of antepartum bleeding episodes, birth weight, male fetus, 5 min APGAR score, arterial pH, postnatal NICU admission, and length of NICU stay. PAS severity was classified as Grade 1, Grade 2, Grade 3 A, Grade 3B, and Grade 3 C [20]. All cases had complete clinical and perinatal data available for analysis.
Outcome
The primary outcome of this study was to evaluate the alignment between the standardized delivery algorithm and gestational age at delivery in PAS cases.
Secondary outcomes included the last cervical length, delivery type (elective vs. urgent), PAS grade, maternal surgical interventions (cystotomy, ureteral injury), number of pRBC, admission to ICU, and neonatal outcomes such as birth weight, NICU admission, and length of NICU stay.
Statistical analyses
All continuous variables were tested for normality using the Shapiro-Wilk test. Normally distributed variables were presented as mean ± standard deviation and compared using an independent t-test. Non-normally distributed variables were reported as median (Q1–Q3) and compared using the Mann-Whitney U test. Categorical variables were expressed as frequencies (%) and compared using the Chi-square test or Fisher’s exact test, as appropriate. Both univariate and multivariate logistic regression analyses were performed to identify factors associated with urgent delivery. Univariate analysis (crude) was first conducted for each variable individually. In the multivariate logistic regression model, the number of antepartum bleeding episodes and last cervical length were included as covariates to determine independent predictors. Crude and adjusted odds ratios (ORs) with 95% confidence intervals (CIs) were reported. Receiver operating characteristic (ROC) curve analysis was performed to evaluate the predictive performance of cervical length, number of antepartum bleeding episodes, and their combination. The statistical analysis was conducted using SPSS software (version 29.0, IBM Corp., Armonk, NY, USA). Microsoft Excel (Microsoft Corporation, Redmond, WA) was used for data organization. Statistical significance was defined as a p-value < 0.05.