Study setting, design and period
This retrospective study was conducted at DR-TB TICs located in Addis Ababa, the capital city of Ethiopia.
According to the Central Statistical Agency’s (CSA) population projection, Addis Ababa has a population size of 3.6 million [19]. It has 11 sub-cities and 123 woredas, with 13 public and more than 25 private hospitals.
St. Peter’s and Alert Comprehensive Specialized Hospitals are the only DR-TB TICs in the city.
St. Peter’s specialized hospital was established in 1953. In the 1960 s, the hospital was the first TB treatment and training center in Ethiopia. It was the first DR-TB TIC in Ethiopia. The TIC has 40 beds.
Alert comprehensive specialized hospital was established in 1934. It was the second DR-TB TIC in Addis Ababa. The TIC has 24 beds.
Data was collected from September 20 to October 15, 2022.
Study participants and sampling procedures
Study participants were adults ((age ≥ 18 years) with RR/MDR-TB treated both at Alert and St. Peter’s Specialized Hospitals. Data was extracted retrospectively among patients treated from January 2016 to April 2022.
First, the total number of MDR/RR-TB patients within the study period was obtained from both Alert (n = 380) and St. Peter’s (n = 535) specialized hospitals. The sample size was allocated proportionally; it was 138 and 193 for Alert and St. Peter’s specialized hospitals, respectively. Seven charts without baseline CXRs were excluded from the study (six and one for Alert and St. Peter’s specialized hospitals, respectively). The data was collected from 324 charts.
Operational definition
Drug-resistant TB is resistant to either or both first-or SL-anti-TB drugs confirmed by drug susceptibility testing (DST).
Rifampicin-mono resistant TB: resistance to rifampicin detected using phenotypic or genotypic methods, with or without resistance to other FL-anti-TB drugs except isoniazid.
Multidrug-resistance (MDR): resistance to at least isoniazid and rifampicin.
Anemia: When hemoglobin level is < 12 g/dL for women and < 13 g/dL for men.
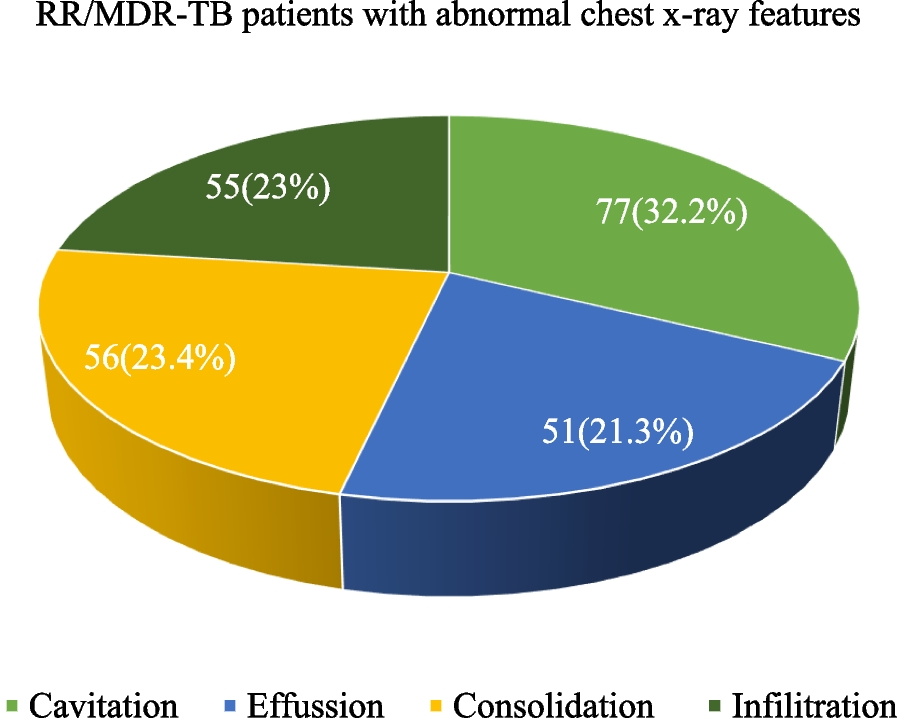
Abnormal chest x-rays: are defined as the presence of nodules, cavities, infiltrations, fibrosis, consolidations, fluid collections, masses, enlarged hilar lymph nodes, narrowing or compression of large airways, opacity in lung tissue, miliary mottling, pleural effusion, pericardial effusion, and abnormality of the thoracic vertebra [12, 20].
Normal chest x-ray: is the absence of abnormal CXR findings.
Comorbidities: presence of medical conditions like diabetes mellitus, hypertension, kidney diseases, liver diseases, asthma, heart diseases, and others in addition to DR-TB [21].
Data collection procedure and quality assurance
Data was extracted using a well-organized checklist containing socio-demographics, clinical, chest x-rays, and laboratory variables. The data was collected by reviewing charts, registration books, green cards, and medical profiles of patients.
Before the actual data collection, a preliminary chart review was done to check the quality of the data collection tool at the University of Gondar Comprehensive Specialized Hospital, DR-TB TIC. Based on the feedbacks obtained from the preliminary review, we updated the data collection checklist.
Three data collectors and one supervisor with previous experience were assigned to each DR-TB TIC. Prior to the data collection, training was given for data collectors and supervisors.
Data entry and analysis
Data completeness and consistency were checked first. The data was entered using Epi Data version 4.1 and then exported to SPSS version 25 for data cleaning and analysis. Descriptive statistics were used to summarize the data using tables and figures. For continuous variables, normality distribution tests were computed using both statistical and normality plot tests; the data was not normally distributed. The Hosmer and Lemeshow goodness-of-fit tests were performed; the binary logistic regression model was a good fit at a P-value of 0.85. The binary logistic regression model was computed to identify factors associated with abnormal CXR features. Bivariate logistic regression analysis was done first to control the effect of confounders, then variables with a p-value < 0.2 were taken into the multivariate logistic regression analysis. Variables with a P-value < 0.05 were considered statistically significant.