Global trends in incidence, prevalence, mortality, and DALY rate of acute and chronic hepatitis C among women aged 15-49 years: 1990–2021
Overview of global trends
As shown in the Table 1, the number of incident cases increased from 29,441,837 in 1990 to 34,003,793 in 2021, representing an increase of approximately 15.5%. The prevalence rate is the same as the incidence rate, indicating that the prevalence of chronic HCV is also increasing. The number of deaths increased from 22,564 in 1990 to 28,584 in 2021, an increase of approximately 26.6%. The DALY rate increased from 1,181,155 in 1990 to 1,485,867 in 2021, an increase of approximately 25.8%.For global acute hepatitis C in 2021, the number of incident cases increased from 652,543 in 1990 to 931,188 in 2021, an increase of approximately 42.7%. The number of prevalent cases increased from 75,293 in 1990 to 107,445 in 2021, an increase of approximately 42.7%. However, the number of deaths decreased from 1,788 in 1990 to 1,348 in 2021, a decrease of approximately 24.6%. The DALY rate number decreased from 103,439 in 1990 to 75,675 in 2021, a decrease of approximately 26.8%(Table 2).
From 1990 to 2021, there was a notable decline in the age-standardized incidence rate (ASIR), prevalence, mortality rate, and disability-adjusted life year (DALY) rate for both acute and chronic hepatitis C virus (HCV) infection among women aged 15-49 years globally.From 1990 to 2021, global chronic HCV burden declined: ASIR fell from 33.156 (95% UI: 17.656, 54.894) to 29.921(95% UI: 15.986, 49.299) per 100,000, ASPR from 2233.253(95% UI: 1763.064, 2753.864) to 1735.267(95% UI: 1344.929, 2164.566), ASMR from 1.905(95% UI: 1.357, 2.535) to 1.417(95% UI: 1.014, 1.885) per 100,000, and DALYs from 97.815 (95% UI: 69.392, 131.017) to 74.071 (95% UI: 52.548, 99.315). Acute HCV also decreased: ASIR dropped from 50.164 (95% UI: 26.974, 82.258)to 47.369 (95% UI: 25.674, 76.832) per 100,000, ASPR from 5.788 (95% UI: 3.112, 9.491) to 5.466 (95% UI: 2.962, 8.865) per 100,000, ASMR from 0.140 (95% UI: 0.023, 0.254) to 0.068 (95% UI: 0.022, 0.132) per 100,000, and DALYs from 7.891 (95% UI: 1.376, 14.251) to 3.857 (95% UI: 1.294, 7.467). EAPCs for ASIR and ASMR were −0.273 and −0.984 for chronic HCV, and −0.164 and −2.478 for acute HCV, respectively.
Regional analysis
In 2021, Central Sub-Saharan Africa had the highest age-standardized incidence rate (ASIR) for chronic HCV at 93.507 (95% UI: 50.934, 150.801) per 100,000, while East Asia had the lowest at 10.840 (95% UI: 4.984, 19.848) per 100,000. Central Asia recorded the highest age-standardized prevalence rate (ASPR) at 6145.910 (95% UI: 4938.906, 7491.315) per 100,000, with Southern Latin America having the lowest at 548.275 (95% UI: 413.864, 703.778) per 100,000. Eastern Europe had the highest age-standardized mortality rate (ASMR) at 2.526 (95% UI: 1.642, 3.741) per 100,000, with an estimated annual percentage change (EAPC) of 4.170 (95% CI : 2.888, 5.468), whereas East Asia had the lowest ASMR at 0.133 (95% UI : 0.081, 0.207) per 100,000. From 1990 to 2021, Eastern Europe saw increases in ASMR and DALY rates for chronic HCV, with EAPCs of 4.170 (95% CI : 2.888, 5.468) and 4.232 (95% CI : 2.928, 5.553), respectively. In contrast, acute HCV mortality and DALY rates declined overall, with East Asia experiencing the fastest decreases, showing EAPCs of −5.114 (95% CI : −5.260, −4.968) and −5.016 (95% CI : −5.159, −4.874), respectively.For acute HCV in 2021, both the ASIR and ASPR were highest in Central Sub-Saharan Africa, at 141.437 per 100,000 (95% UI: 78.217, 226.542) and 16.320 per 100,000 (95% UI: 9.025, 26.139), respectively. The lowest ASIR and ASPR were observed in East Asia, at 16.914 per 100,000 (95% UI: 7.896, 30.567) and 1.952 per 100,000 (95% UI: 0.911, 3.527), respectively (Supplementary Table 2).
Sociodemographic Index (SDI) analysis
Based on SDI levels, the 204 countries and territories were divided into five categories: low SDI (<0.46), low-middle SDI (0.46–0.60), middle SDI (0.61–0.70), upper-middle SDI (0.71–0.80), and high SDI (>0.81). In 2021, the burden of chronic HCV among women aged 15-49 years was most severe in the low SDI level, with an ASIR of 49.841 per 100,000 (95% UI: 26.711, 81.663) and an ASPR of 2410.594 per 100,000 (95% UI: 1864.624, 3015.041). The lowest ASIR and ASMR were found in the upper-middle SDI level, at 19.735 per 100,000 (95% UI: 10.405, 33.084) and 0.702 per 100,000 (95% UI: 0.471, 1.001), respectively. The lowest ASPR was observed in the high SDI level, at 872.222 per 100,000 (95% UI: 667.595, 1103.395). For acute HCV, the burden was heaviest in the low SDI level, with an ASIR of 76.069 per 100,000 (95% UI: 41.357, 123.570) and an ASPR of 8.777 per 100,000 (95% UI: 4.772, 14.258) (Supplementary Table 1 and Supplementary Table 2).
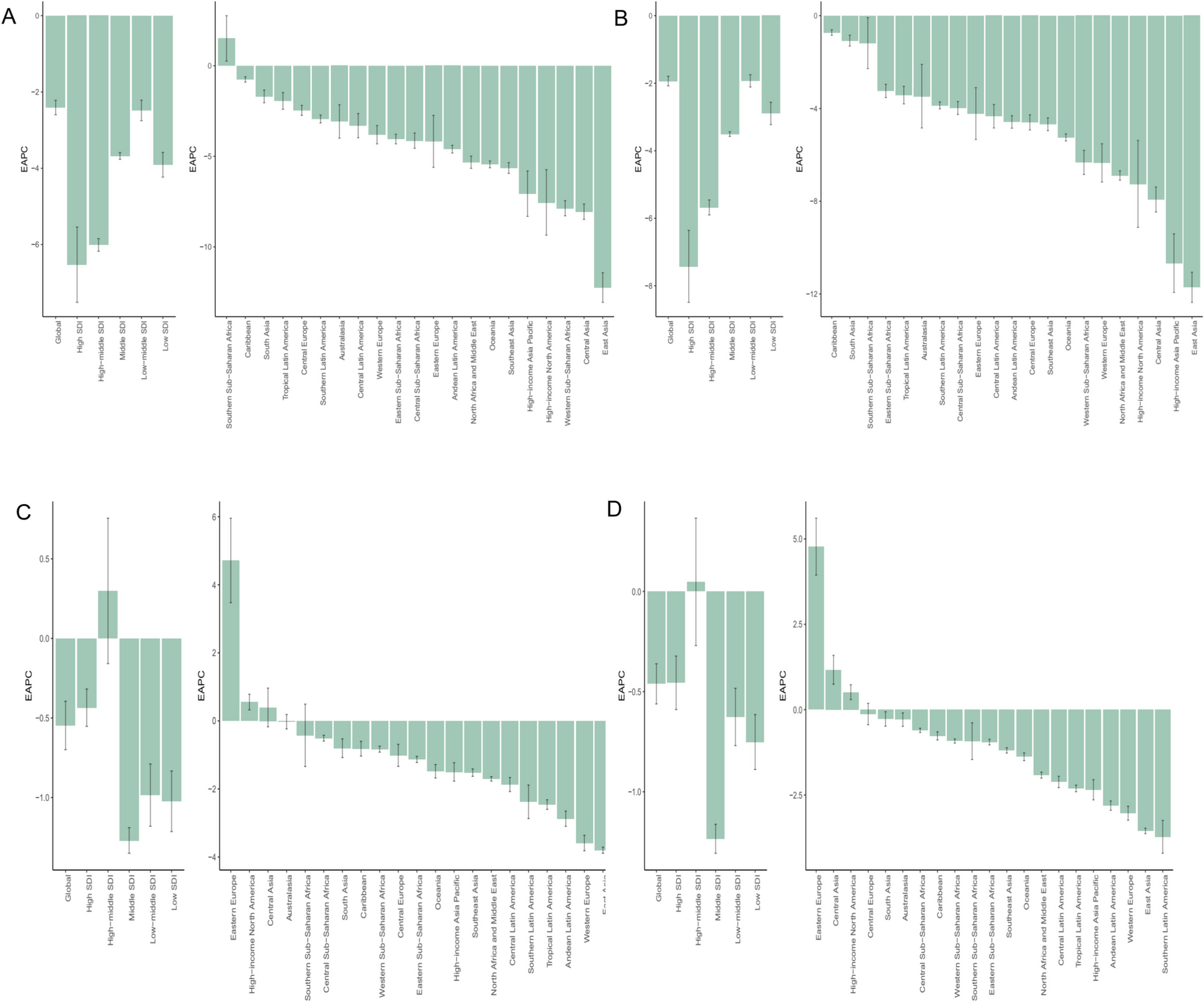
From 1990 to 2021, the ASMR and DALY rate for chronic HCV decreased most rapidly in the middle SDI level, with EAPCs of −1.966 (95% CI: −2.029, −1.903) and −1.946 (95% UI: −2.012, −1.880), respectively. For acute HCV, the ASMR and DALY rate decreased most significantly in the high SDI level (Fig. 1).
Estimated Annual Percentage Change (EAPC) of Mortality and DALY rates for Acute and Chronic HCV Among Women Aged 15-49 Years A:Mortality of Acute. HCV;B:DALY rates of Acute HCV;C:Mortality of Chronic HCV;D:DALY rates of Chronic HCV
The global heat maps reveal substantial disparities in the disease burden of acute and chronic hepatitis C virus (HCV) across countries and regions(Fig. 2 and Supplementary Figure 1). Supplementary Table 3 and Supplementary Table 4 provide a detailed ranking of the top 20 countries or regions with the highest mortality rates for acute and chronic HCV in 2021, including age-standardized incidence rates (ASIR), prevalence rates (ASPR), mortality rates (ASMR), disability-adjusted life year (DALY) rates, and estimated annual percentage changes (EAPC) from 1990 to 2021.
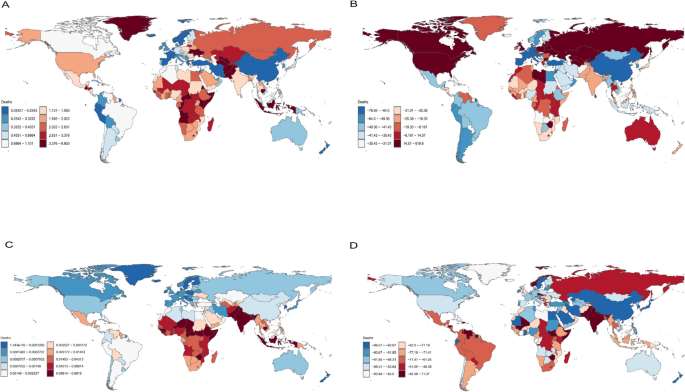
Global heat maps illustrating the disease burden of acute and chronic hepatitis C virus(HCV) infection among women aged 15-49 years in 2021A: Age-Standardized Mortality Rate(ASMR) for Chronic Hepatitis C in 2021;B: Estimated Annual Percentage Change (EAPC) inChronic Hepatitis C Mortality Rates, 1990–2021;C: Age-Standardized Mortality Rate(ASMR) for Acute Hepatitis C in 2021;D: Estimated Annual Percentage Change (EAPC) inAcute Hepatitis C Mortality Rates, 1990–2021
In 2021, Pakistan bore the heaviest burden of chronic HCV, with an ASMR of 6.6 (95% UI: 3.89, 10.38) and an ASDR of 360.36 (95% UI: 211.72, 568.35). Turkmenistan followed closely with an ASMR of 5.93 (95% UI: 3.07, 9.6) and an ASDR of 306.54 (95% UI: 157.67, 501.11). In contrast, the Cook Islands had the lowest burden, with an ASMR of 0.02 (95% UI: 0.009, 0.05) and an ASDR of 1.45 (95% UI: 0.58, 2.96).
From 1990 to 2021, among the 204 countries and territories analyzed, the Russian Federation showed the most significant upward trend in ASMR, with an EAPC of 6.19 (95% CI: 5.24, 7.19).For acute HCV in 2021, Pakistan again topped the list with an ASMR of 0.68 (95% UI: 0.08, 1.63) and an ASDR of 34.77 (95% UI: 4.36, 83.39). The Cook Islands had the lowest burden, with an ASMR of 0.02 (95% UI: 0.009, 0.05) and an ASDR of 1.45 (95% UI: 0.58, 2.96).Over the same period, Norway experienced the most significant increase in ASMR for acute HCV, with an EAPC of 0.71 (95% CI: 0.24, 1.4).
Association between the burden of acute and chronic hepatitis C among women of reproductive age and SDI levels across 21 geographic regions, 1990–2021
Between 1990 and 2021, the burden of hepatitis C virus (HCV) infection among women of reproductive age was closely linked to regional sociodemographic development. Measured by age-standardized incidence rate (ASIR), prevalence rate (ASPR), mortality rate (ASMR), and disability-adjusted life year rate (ASDR), the burden of chronic HCV generally decreased as Sociodemographic Index (SDI) values increased across almost all regions(Fig. 3). However, Central Asia emerged as an exception, maintaining a higher ASPR despite improvements in its SDI. In contrast, for acute HCV, the most significant declines in ASMR and ASDR were observed in low-SDI regions, while these metrics remained largely stable in other areas. Notably, North Africa and the Middle East exhibited higher ASIR and ASPR than other regions.
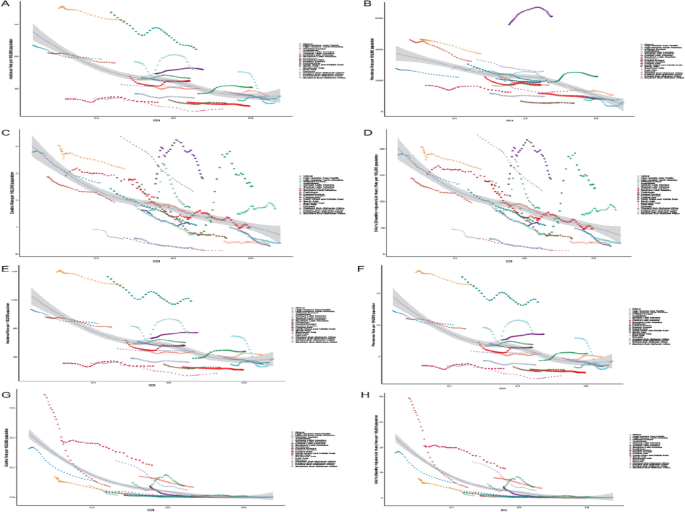
The solid line illustrates the nonlinear relationship between the Sociodemographic Index (SDI) and the burden of hepatitis C disease(chronic and acute)across 21 GBD-defined regions, in 2021.A:ASIR for chronic hepatitis C(R=−0.4711,P<0.001) B:ASPR for chronic hepatitis C (R=−0.6774,P<0.001)C:ASMR for chronic hepatitis C (R=−0.5177,P<0.001)D:ASDR for chronic hepatitis C(R=−0.5122,P<0.001) E:ASIR for acute hepatitis C(R=−0.4634,P<0.001) F:ASPR for acute hepatitis C(R=−0.4634,P<0.001) G:ASMR for acute hepatitis C(R=−0.8274,P<0.001) H:ASDR for acute hepatitis C(R=−0.8262,P<0.001)
From 1990 to 2021, there was a notable inverse relationship between increasing SDI levels and the burden of chronic HCV among women of reproductive age. As regions progressed socioeconomically, represented by rising SDI scores, the ASIR, ASPR, ASMR, and ASDR for chronic HCV generally declined. This trend underscores the positive impact of socioeconomic development on reducing disease burden. However, Central Asia stood out with persistently higher ASPR, indicating unique regional challenges that may require targeted interventions.
For acute HCV, regions with lower SDIs experienced the most pronounced decreases in ASMR and ASDR over the study period. This suggests that improvements in healthcare infrastructure, early diagnosis, and treatment access in less developed regions have significantly impacted acute HCV mortality and morbidity. Meanwhile, other regions saw little change in their ASMR and ASDR, emphasizing the need for sustained efforts to address acute HCV effectively.
To investigate the factors influencing the estimated annual percentage change (EAPC), we analyzed the relationships between EAPC and the ASMR and ASDR for both acute and chronic HCV infections in 2021. Additionally, we explored the association between EAPC and the SDI levels of countries in 2021(Supplementary Figure 2).
Our analysis revealed several key findings:Chronic Hepatitis C: There was a significant positive correlation between EAPC and the ASMR for chronic HCV in 2021 (ρ=2.7 ×10^−16, P<0.001), as well as with the ASDR (ρ=3.7×10^−13,P<0.001). Conversely, EAPC showed a significant negative correlation with SDI levels in 2021 (ρ = −0.00017,P<0.001). These results suggest that regions with higher EAPCs experienced greater increases in chronic HCV mortality rates over time, while improvements in SDI were associated with decreasing EAPCs.
Acute Hepatitis C: For acute HCV, there was also a significant positive correlation between EAPC and the ASMR in 2021 (ρ=7.8×10^−8,P<0.001). Similar to chronic HCV, EAPC for acute HCV exhibited a significant negative correlation with SDI levels (ρ=−2.8×10^−10,P<0.001). This indicates that regions with higher EAPCs saw an increase in acute HCV mortality rates, whereas higher SDI levels were linked to lower EAPCs.
North Africa and the Middle East consistently reported higher ASIR and ASPR for both acute and chronic HCV among women of reproductive age compared to other regions. Factors such as higher transmission rates, limited preventive measures, or differences in healthcare system effectiveness may contribute to this pattern. The region’s distinct epidemiological profile calls for tailored strategies to control and reduce HCV incidence and prevalence.
The analysis from 1990 to 2021 reveals a complex interplay between SDI levels and the burden of acute and chronic HCV among women of reproductive age. While improvements in SDI are generally associated with reduced HCV burden, certain areas like Central Asia and North Africa and the Middle East exhibit unique patterns. Continued monitoring and adaptive public health policies will be essential in addressing the ongoing challenges posed by HCV globally, particularly among vulnerable populations. The strong correlations found provide valuable insights into the effectiveness of past interventions and inform future strategies to combat HCV, highlighting the importance of sociodemographic development in mitigating the impact of HCV-related mortality.
Global trends in age-standardized incidence and mortality rates of acute and chronic hepatitis C among women aged 15-49 years (1990-2021)
Figure 4 and Supplementary Figure 3 illustrates the temporal trends in age-standardized incidence and mortality rates of chronic hepatitis C among women aged 15-49 years globally from 1990 to 2021. Overall, both incidence and mortality rates exhibited a declining trend. Specifically, the incidence rate showed continuous declines from 1990 to 2000, followed by a slight increase from 2001 to 2005, another decline from 2005 to 2010, and a minor uptick from 2015 to 2021. Mortality rates demonstrated a consistent downward trend, with the most pronounced decrease observed between 2005 and 2021.
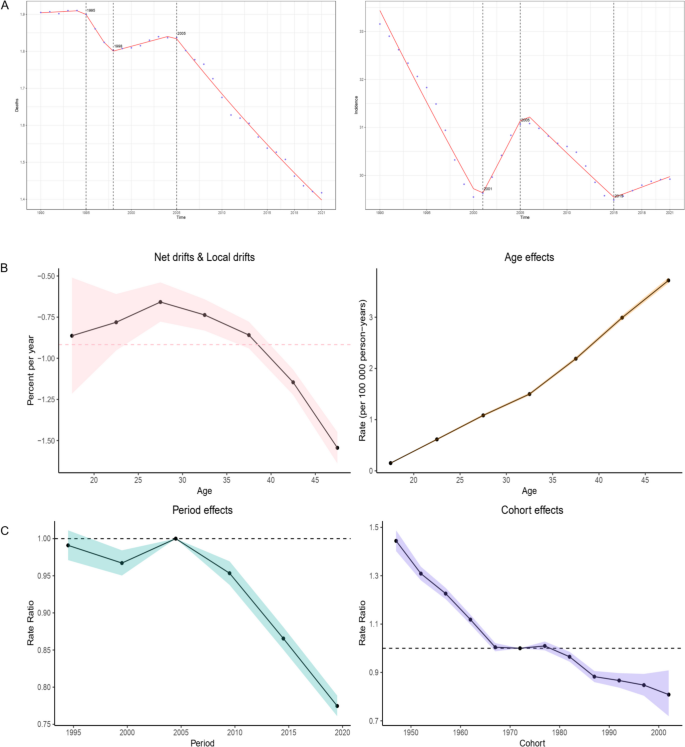
A Trends in Mortality and Incidence (1990-2021)Line plots illustrating the Average Annual Percentage Change(AAPC) for mortality (left panel) and incidence (right panel) of chronic hepatitis C among women of reproductive age(15-49 years) from 1990 to 2021. These plots provide a visual representation of the overall temporal trends in diseaseburden over the three-decade period. B & C Age-Period-Cohort (APC) Analysis of Chronic Hepatitis C Temporal Drifts:The top left panel displays net and local drifts, with values greater than zero indicating an increasing trend in the burden ofchronic hepatitis C. Age Effects: The top right panel examines how different age groups within the reproductive age range contribute to the burden of chronic hepatitis C. Period and Cohort Rate Ratios: The bottom panel presents rate ratios for period and cohort effects; values greater than one suggest an increased burden of chronic hepatitis C associated with specific periods or birth cohorts
The age-standardized incidence trend for acute hepatitis C among women aged 15-49 years mirrored that of chronic cases, including an upward trend from 2015 to 2021. The mortality rate for acute hepatitis C continuously declined throughout the study period.
The age-period-cohort (APC) model fitting for mortality rates of acute and chronic hepatitis C among women aged 15-49 years revealed statistically significant global shifts, local shifts, overall age deviations, overall period deviations, period relative risk (RR) values, cohort RR values, and total cohort deviations for acute hepatitis C (P < 0.05, Supplementary Table 5). However, for chronic hepatitis C mortality, only the overall age deviation and cohort RR values were not statistically significant (P < 0.05, Supplementary Table 6).
The longitudinal age curve for chronic hepatitis C mortality, after adjusting for period and cohort effects, shows an increasing trend with age. From 1990 to 2021, the risk of chronic hepatitis C mortality decreased over time. After correcting for period and age effects, using the 1950-2000 cohort as a reference, the risk of chronic hepatitis C mortality also showed a decreasing trend, with similar observations for acute hepatitis C (Supplementary Figure 3).
BAPC model projections for the global burden of acute and chronic hepatitis C among women aged 15-49 years
The Bayesian Age-Period-Cohort (BAPC) model projects that over the next decade, the global incidence and mortality rates for both acute and chronic hepatitis C among women aged 15-49 years will exhibit a declining trend(Fig. 5). Global epidemiological trends of hepatitis C demonstrate a progressive decline in the age-standardized incidence rate (ASR) of chronic cases from 16.44 (95% CI: 16.39-16.50) in 1990 to a projected 14.29 (14.28-14.30) by 2035, accompanied by a significant mortality reduction from 0.945 (0.933-0.957) to 0.647 (0.632-0.662), with the most pronounced annual decline of 0.012 observed during 2010-2020, reflecting the therapeutic success of direct-acting antivirals (DAAs). While acute cases showed an overall ASR decrease from 24.87 (24.81-24.93) to 22.51 (22.46-22.56), a subtle resurgence (22.99→23.46) during 2010-2020 suggests persistent gaps in high-risk population containment. Acute case mortality demonstrated the most rapid decline from 0.0704 (0.0679-0.0728) to 0.0214 (0.0175-0.0253), with maximum annual reduction of 0.0015 during 2000-2010. Notably, all indicators showed progressive narrowing of 95% confidence intervals (e.g., chronic incidence CI width reduced from 0.11 to 0.02), indicating continuous improvements in surveillance systems and predictive modeling. However, relatively expanded uncertainty in long-term mortality projections (CI width increased from 0.0049 to 0.0078) underscores the necessity to enhance screening for high-risk populations and interventions in resource-limited regions while maintaining current control measures, addressing challenges during the plateau phase to ultimately achieve WHO’s strategic goal of viral hepatitis elimination.This forecast underscores a significant public health achievement in reducing the impact of hepatitis C on this demographic group. Notably, despite the anticipated decrease in rates, the absolute number of new cases is expected to rise annually over the coming ten years. This paradox can be attributed to the growing global population of women within this age range, leading to an increase in the total number of individuals at risk. The BAPC model’s predictions highlight the importance of continued surveillance and targeted interventions to mitigate the rising caseload, even as the disease’s relative burden diminishes. Policymakers and healthcare providers should prepare for these challenges by strengthening prevention programs, enhancing early detection efforts, and expanding access to effective treatments. These actions are crucial to ensuring sustained progress in combating hepatitis C and protecting the health of women of reproductive age globally.
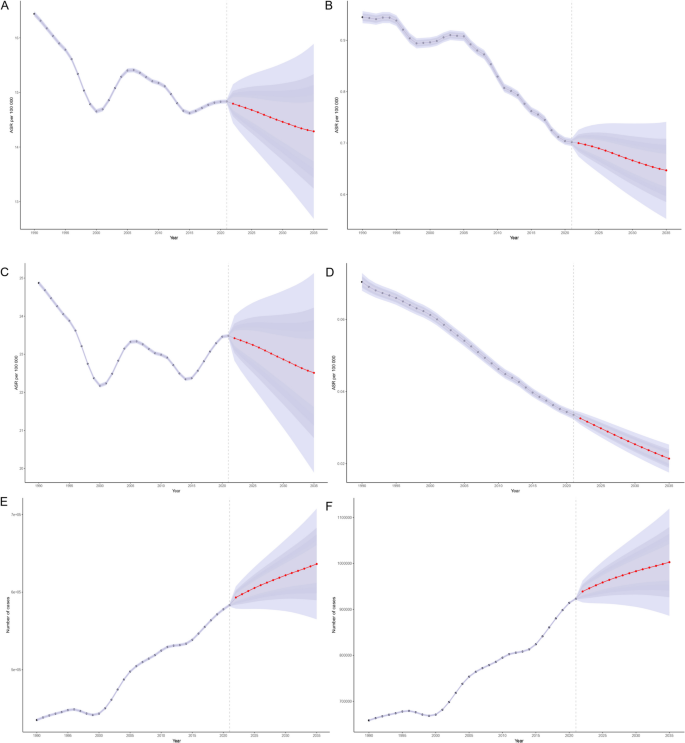
Predictions of Age-Standardized Rates (ASR) and Absolute Numbers for Mortality, Incidence of Acute and Chronic Hepatitis C.This figure presents projected trends for acute and chronic hepatitis C in terms of age-standardized incidence rates (ASIR), age-standardized mortality rates (ASMR), and absolute numbers of new cases: A:ASIR Trends for Chronic Hepatitis C: Projected changes in age-standardized incidence rates.B:ASMR Trends for Chronic Hepatitis C: Projected changes in age-standardized mortality rates.C:ASIR Trends for Acute Hepatitis C: Projected changes in age-standardized incidence rates.D:ASMR Trends for Acute Hepatitis C: Projected changes in age-standardized mortality rates.E:Number of New Cases of Chronic Hepatitis C: Projected trends in the absolute number of new chronic cases.F:Number of New Cases of Acute Hepatitis C: Projected trends in the absolute number of new acute cases
Decomposition analysis of acute and chronic hepatitis C incidence among childbearing-age females: global trends and regional variations
The decomposition analysis of acute and chronic hepatitis C (HCV) incidence among females of childbearing age reveals significant global trends and regional disparities. Globally, both acute and chronic HCV cases have increased, underscoring the complex interplay of demographic, structural, and epidemiological factors that vary across regions (Fig. 6).
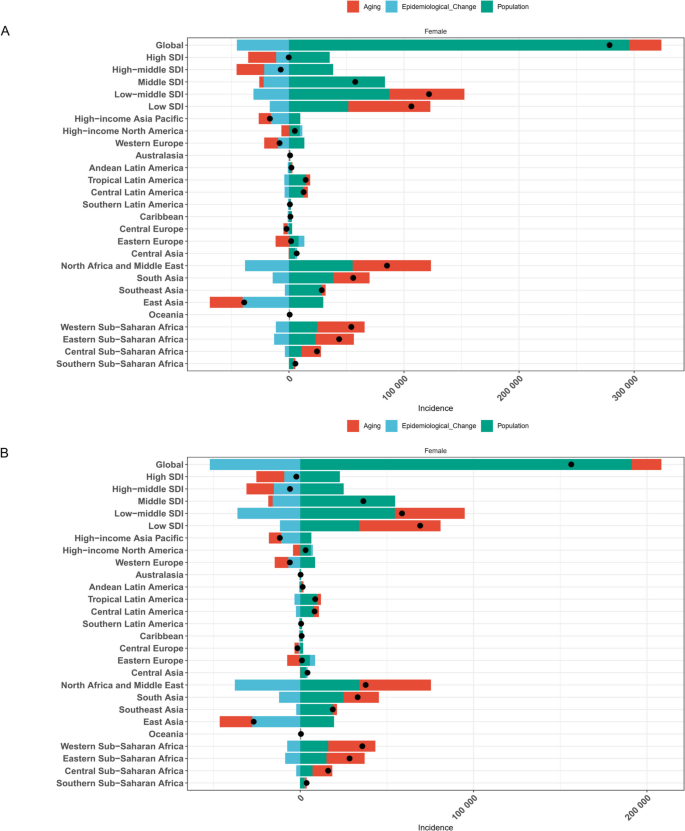
Decomposition of Changes in New Cases of Acute and Chronic Hepatitis C (1990-2021)A: Acute Hepatitis C;B: Chronic Hepatitis C This figure decomposes the changes in the number of new cases of acute and chronic hepatitis C into contributions from:Population Growth (Green): Increase due to overall population expansion.Population Ageing (Red): Changes attributable to shifts in age structure.Epidemiological Changes (Blue): Variations due to disease transmission rates, healthcare improvements, and public health interventions.Black dots represent the total change contributed by all three components. Positive values indicate an increase in incidence, while negative values indicate a decrease. The analysis is conducted globally and across various Sociodemographic Index (SDI) regions
Regional trends in acute HCV incidence exhibit contrasting patterns. East Asia has seen a notable decline, likely attributable to robust public health interventions and medical advancements. Conversely, Sub-Saharan Africa and Low Socio-Demographic Index (SDI) countries have experienced rising incidences, reflecting challenges in healthcare access and socio-economic conditions. The dynamics of aging populations, changes in population structure, and epidemiological transitions significantly influence these trends, with varying impacts observed across different regions.
Chronic HCV incidence has also risen globally, with particularly marked increases in North Africa and the Middle East. High-income Asia Pacific regions, however, have witnessed reductions, possibly due to rapidly aging populations which generally contribute negatively to new chronic HCV infections. Yet, this trend can be counterbalanced by population growth or migration in certain areas, highlighting the nuanced impact of demographic shifts on disease prevalence.
Key Influencing Factors:Aging Populations: Regions with older demographics tend to experience fewer new acute HCV infections but mixed impacts on chronic HCV incidence.Population Structure Changes: Growth in younger populations, such as in Sub-Saharan Africa, contributes to higher HCV incidence rates.Epidemiological Changes: Emergence of new risk factors or improvements in disease control—such as enhanced healthcare infrastructure in Central Latin America—significantly affect HCV incidence.
In conclusion, the decomposition analysis underscores the multifaceted nature of HCV incidence among childbearing-age females. It highlights the need for tailored public health strategies that address region-specific challenges. Continued monitoring and adaptive health policies are crucial for effectively managing the global burden of hepatitis C. This analysis provides valuable insights into the diverse dynamics of HCV incidence, informing targeted interventions to mitigate its impact worldwide.