
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson from the Yale School of Medicine.
I am 45 years old. And I have been 45 years old for 8 months now. And I’m a doctor. A doctor who prides himself on being up to date on medical guidelines, practices, and evidence. And you know what I have not done yet? Not even made an attempt to do yet? Scheduled my screening colonoscopy.
Let me be clear, this is not out of some high-minded concern for overdiagnosis or the issue of false positives in screening exams. This is pure, unadulterated, laziness. Or perhaps, if I’m being generous, I simply have too many other things going on in my life to take the 20 minutes to get this thing scheduled.
I probably should, because the rate of colorectal cancer among people ages 45-49 has been going up steadily since at least the mid-90s and dramatically over the last few years. We need to figure out what’s going on.
We’re going to dig into the rising incidence of so-called “early onset” colon cancer in a minute, but let me point out that, in recognition of the changing demographics of the disease, the United States Preventive Services Task Force (yes, that same USPSTF that may soon be fired en masse by RFK Jr) changed their recommended starting screening age from 50 to 45 years of age in 2021.
With a stroke of a pen, 45 million Americans were suddenly eligible for colon cancer screening, typically through colonoscopy or a fecal immunochemical test: that’s the one you do at home that lets you know if there is microscopic blood in your stool.
And now, 4 years later, we can look back and see the effect that change in screening criteria had. In fact, appearing this week in JAMA, we have a trio of papers looking at the issue of early-onset colorectal cancer from a few different angles: How to get younger people like me to screen, how much younger people like me are screening, and how much new colon cancer we are detecting.
Let’s start with the screening numbers. In Trends in Colorectal Cancer Screening in US Adults Aged 45 to 49 Years, Jessica Star at the American Cancer Society and colleagues used a nationally-representative health survey to look at screening across various age groups and over time.
The primary results are here.
You can see that screening is pretty rare among 40–44-year-olds and hasn’t changed much over time. That seems right; guidelines currently suggest to start screening at 45, not 40.
Moving into my age group, you see a dramatic increase from about 20% screening in 2019 and 2021 to 35% screening in 2023.
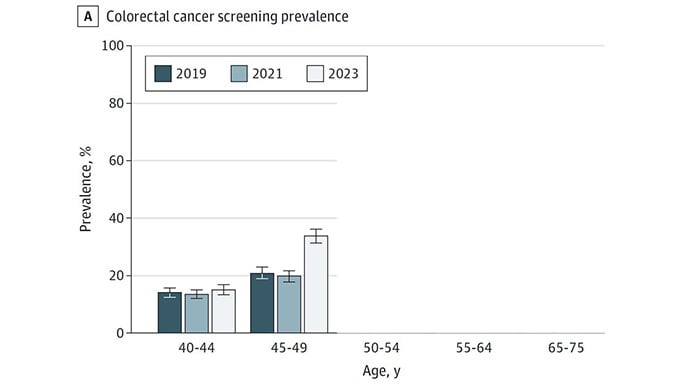
This is about a 60% relative increase in baseline screening rates. It’s not perfect, of course. People like me who haven’t gotten around to screening yet are still in the majority, but it shows how guideline changes can move the needle on this stuff. Of course, it’s worth noting that the Affordable Care Act (Obamacare) mandates that insurers cover any screening test recommended by the USPSTF. Paying for screening also increases screening.
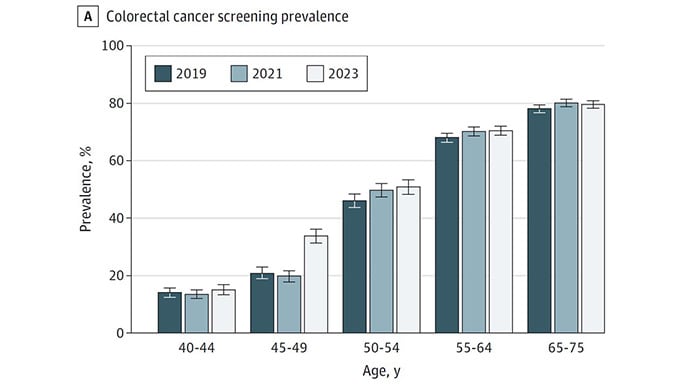
One concern people had about the change in guidelines was that all this new screening in younger people would crowd out screening in older people. The data, fortunately, doesn’t show this. Screening rates were high and stable in the over 50 crowd over the past 5 years.
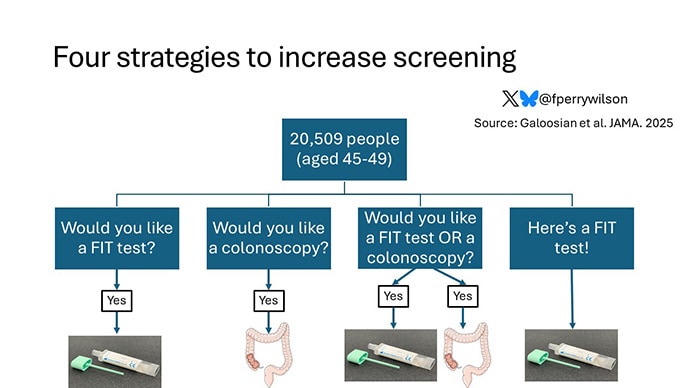
If you’re a believer in screening, you probably want to know how to improve rates among younger people like me. In another article in this week’s JAMA, researchers led by Artin Galoosian at UCLA report out results from a randomized trial that tried four different strategies to increase the screening rate in people aged 45-49.
A bit more than 20,000 individuals were randomized. A quarter of them were invited, via an online patient portal, to use the fecal immunochemical test (FIT) for screening. Another quarter were invited to do a screening colonoscopy. A quarter were invited to do either; they could choose which they preferred. And, finally, a quarter were simply mailed a FIT.
Of the people invited to do FIT testing, 18% got some kind of screening, mostly colonoscopy.
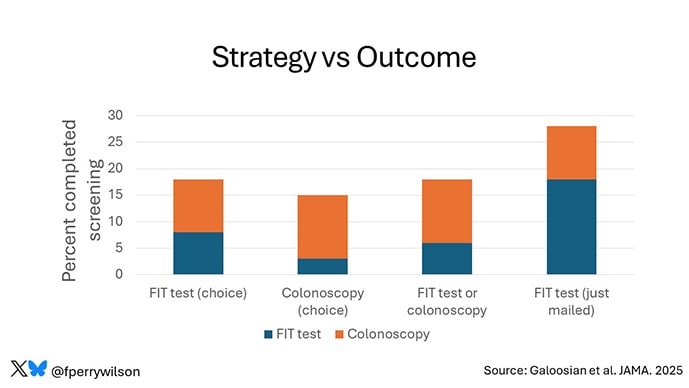
Of those invited to colonoscopy, 15% were screened. Of those given the choice between the two, 18% picked one or the other. But in those who just had the test show up in the mail, 28% completed screening. This is pretty powerful data. It confirms a fundamental principle of behavioral economics: People will do something if you make it easy for them.
Anecdotally, if I opened the mail tomorrow and a FIT test was in there, I’m pretty sure I would do it. Since that isn’t standard of care (yet), I need to call my PCP (who I haven’t seen in like 5 years) and go through the rigamarole. But I’ll do it. I will. I think.
Now, I opened this commentary by mentioning that all of this research is driven by the simple observation that colorectal cancer rates are increasing in young people. A third paper in JAMA this week, Colorectal Cancer Incidence in US Adults After Recommendations for Earlier Screening, from Elizabeth Schafer and colleagues at the American Cancer Society, tracks those rates for us from 2006 on using the SEER database.
There are some really interesting findings here. Let me start with this picture, the rate of any colon cancer diagnosis in individuals aged 45-49. You see a steady uptick, about 1% per year from 2006 on, and then a dramatic increase (about 12%) in the past few years.
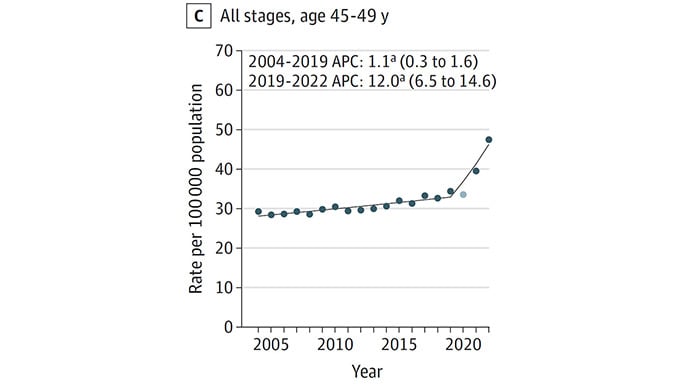
That’s a scary graph. But I’ll de-scare it a bit for you. Here is the graph for local colorectal cancer over that time period. These are early cancers that have not yet spread.
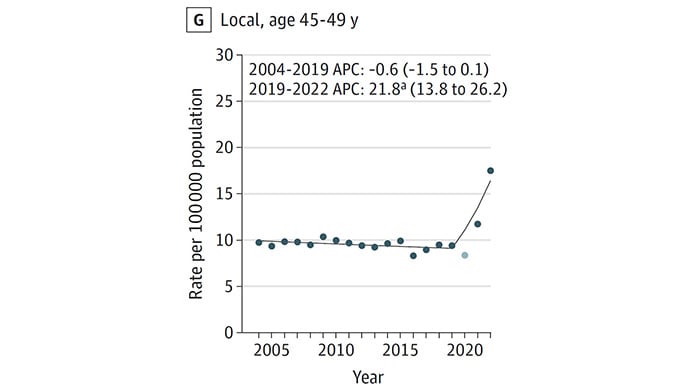
It looks very similar. In fact, according to the paper, nearly all of that accelerated increase in the past few years is driven by early, local cancers. That is a strong signal that it is the increased screening that is leading to increased diagnosis, as opposed to some new environmental or other exposure. And, since early cancers are more treatable, we can potentially argue that this increase is actually a good thing. Better to detect now than later.
But the rise in [colorectal cancer] in young people is not all due to screening. Here is the graph showing the rate of colorectal cancer with distant metastases over time.
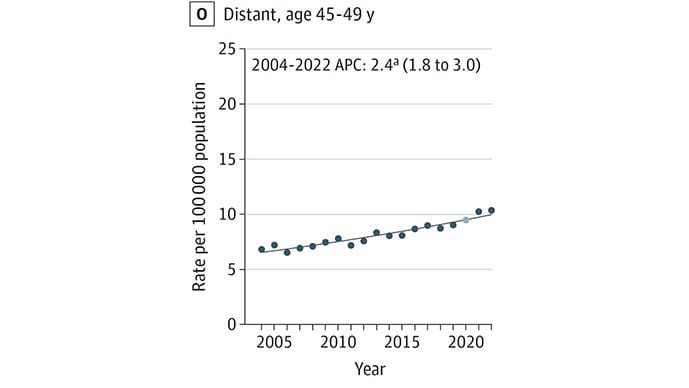
You see a steady increase — no big inflection that we can attribute to more screening. Nor would you expect there to be, as screening is really optimized to catch early cancers, not metastatic ones.
Bottom line: If you hear headlines about a startling rise in colorectal cancer in young people, realize that there is nuance here. Yes, there has been a dramatic rise in the last few years, mostly because we are catching early cancers through screening. But there has also been a slower rise over a much longer time period. Over decades.
Which leaves the question of… why? Why is colon cancer affecting younger and younger people over time? What has changed in our lives during the past 30 years? There is no smoking gun, but there are an awful lot of possibilities. I think the obesity epidemic is a big one here, and it will be interesting to see if these curves flatten in the GLP-1 era. But there are other possibilities: microbiome changes, ultraprocessed foods, even microplastics. It will take a bit more detailed epidemiology to get to the bottom of the increased risk in younger people. But, given the data, well, I should probably call my PCP and get that damn colonoscopy scheduled.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here on Medscape. He posts at @fperrywilsonand his book, How Medicine Works and When It Doesn’t, is available now.