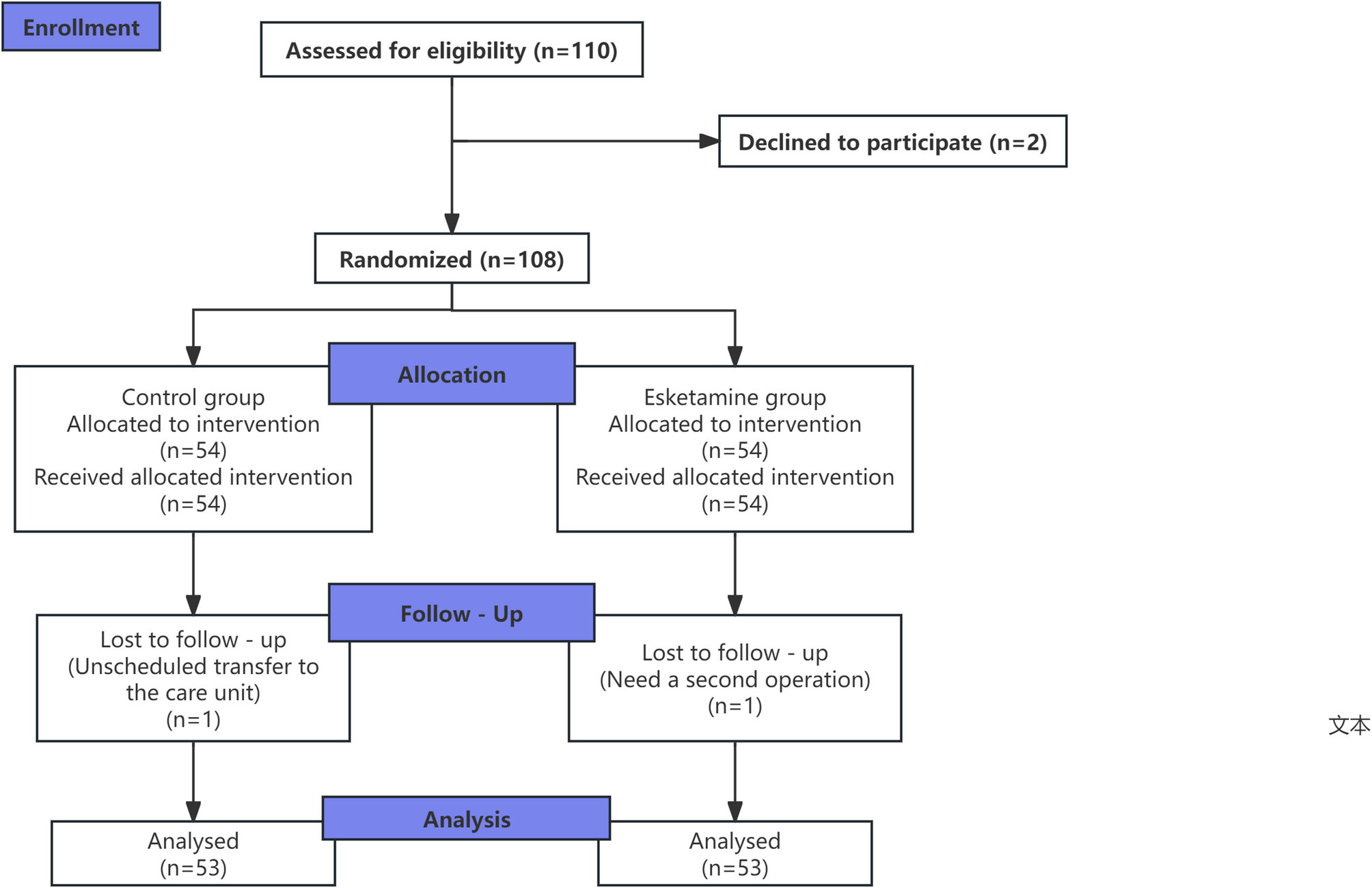
In this randomized controlled trial, we aimed to evaluate the effect of low-dose esketamine on POD in 108 older patients with fragile brain function undergoing thoracoscopic lung cancer surgery. Patients were randomly assigned to receive either esketamine (0.25 mg/kg during induction, 0.1 mg/kg/h for 30 min during maintenance) or normal saline. We found that the esketamine group had a significantly lower incidence of POD at 24 h post-surgery (3.8% vs. 15.1%, P = 0.046) but not at 72 h. Serum levels of interleukin-6 and S100β, markers of inflammation, were significantly lower in the esketamine group on the first postoperative day. Additionally, esketamine use was associated with reduced sufentanil consumption, shorter extubation time, recovery room stay, and total hospital stay, as well as higher post-extubation SpO2 and lower rescue analgesia rates, without increasing adverse events like dizziness or nausea. These findings highlight esketamine’s potential to mitigate early POD, inhibit inflammation, and accelerate postoperative recovery in this vulnerable patient population.
Patients with fragile brain function are often complicated by a history of stroke, imaging-confirmed cerebral infarction, cerebral vascular stenosis, alzheimer’s disease, parkinson’s disease, and other conditions. These patients have weaker neural plasticity and recovery capabilities, making them more susceptible to the effects of surgical anesthesia, which leads to a higher incidence of POD. Therefore, this study focuses particularly on this special older population.
Research has shown that sub-anesthetic doses of esketamine may effectively reduce the incidence of delayed neurocognitive recovery and may improve early postoperative cognitive function in older patients undergoing gastrointestinal surgery [10]. Other studies have found that continuous intraoperative infusion of esketamine may help prevent sleep disorders after gynecological laparoscopic surgery, potentially reducing the risk of POD and cognitive dysfunction [15]. This study references the aforementioned literature and, based on preliminary trials, adopted an intravenous bolus dose of 0.25 mg/kg for esketamine and a continuous infusion at 0.1 mg/kg/h for 30 min during surgery.
POD is one of the common and serious complications in older patients, especially for those with fragile brain function, where the incidence and harm are more significant. In this study, compared with the control group, the incidence of POD in the esketamine group was significantly decreased 24 h after surgery, while there was no significant difference in the incidence of POD 72 h after surgery between the two groups. This suggests that a small dose of esketamine may have advantages in preventing early POD, though further research is needed to confirm this effect in broader patient populations. Esketamine may act on multiple receptors such as NMDA, γ-aminobutyric acid (GABA), cholinergic, opioid, and dopamine receptors [16], suggesting potential mechanisms for its effects. Its protective effect on the central nervous system may be a key factor. On the one hand, esketamine may regulate the neurotransmitter system, such as inhibiting the excessive release of excitatory amino acids and stabilizing the membrane potential of nerve cells, thereby reducing the damage and inflammatory response of nerve cells. Research has shown that esketamine may reduce neuroinflammation by regulating the activity of microglia and inhibiting their overactivation, thereby reducing damage to neurons and the release of inflammatory mediators [17], which helps to maintain the stability of brain function to a certain extent and reduce the risk of POD. On the other hand, the analgesic effect of esketamine may indirectly reduce the stress response caused by postoperative pain, and stress response is often an important factor in inducing POD.
Inflammatory response plays an important role in the occurrence and development of POD. Surgical trauma induces a systemic inflammatory response, and inflammatory cytokines can cross the blood-brain barrier and activate microglia, triggering neuroinflammation, which may induce POCD and POD [7] This study found that there was no statistically significant difference in the serum concentration of IL-6 and S100β between the two groups before surgery, but on the first postoperative day, both IL-6 and S100β in the esketamine group were significantly lower than those in the control group.This suggests that esketamine may effectively inhibit the excessive activation of postoperative inflammatory response, though further research is needed to confirm this potential effect. Research has shown [18] that esketamine significantly reduces inflammation levels by regulating the expression of multiple cytokines. As an important inflammatory mediator, IL-6 is released in large quantities after surgical trauma, triggering a systemic inflammatory response, which in turn affects brain function and increases the incidence of delirium. S100β is a sensitive indicator reflecting brain damage and blood-brain barrier disruption. The decrease in its level indicates that esketamine may play a protective role in the microscopic structure of the brain, reducing brain damage caused by surgery and brain function disorders mediated by inflammation, which is consistent with the reduction in the incidence of POD, further revealing that the potential mechanism of esketamine in preventing POD may be closely related to inhibiting inflammatory response and reducing brain damage.
Research has found that esketamine can reduce the consumption of opioid medications during surgery [19]. The results of this study are consistent with previous reports. In this study, the use of sufentanil in the esketamine group and the rate of rescue analgesia in the recovery room were lower than those in the control group, and the esketamine group had a higher SpO2 after extubation compared with the control group. The discrepancy in sufentanil usage between the two groups in this study may be attributed to two key mechanisms. First, during skin incision at the commencement of surgery, supplemental sufentanil (5–10 µg) was administered based on individual stress responses. Esketamine may antagonizes the N-methyl-D-aspartate (NMDA) receptor, possibly inhibits the activation and maintenance of the pain center, and also has a certain µ-receptor antagonistic effect, producing a strong analgesic effect mitigated stress reactions during incision in the esketamine group, thereby potentially reducing the need for sufentanil. Second, esketamine may alleviate postoperative hyperalgesia caused by remifentanil [20, 21], potentially reducing the need for rescue analgesia with sufentanil in the recovery room. Collectively, these factors contributed to lower overall perioperative sufentanil consumption in the esketamine group. In addition, esketamine may directly stimulate the respiratory center, thereby potentially counteracting the respiratory depression induced by opioids [22]. Research has also found that multi-component interventions can effectively reduce the incidence of POD [23], and multimodal analgesia is an important part of this approach. In this study, the esketamine group adopted a multimodal analgesia regimen with esketamine combined with non-steroidal anti-inflammatory drugs and paravertebral nerve block, which reduced the rate of rescue analgesia, decreased the consumption of opioids, and did not increase the incidence of adverse reactions. In terms of postoperative recovery indicators, the postoperative extubation time, recovery room stay time, and total hospital stay in the esketamine group were also shorter than those in the control group. These results suggest that esketamine may be beneficial to the early postoperative respiratory function recovery and rapid rehabilitation of patients and could potentially shorten the hospital stay by reducing postoperative pain and complications, reducing the economic burden on patients and the occupation of medical resources. Its rapid rehabilitation advantage may stem from its regulation of the overall stress response of the body and its effective control of postoperative pain and inflammation, thus creating a more favorable physiological and psychological state for patients’ recovery.
However, this study also has certain limitations. Firstly, the sample size of this study is relatively limited. Although the results are statistically significant, larger-scale multicenter clinical trials are still needed to further verify its reliability and universality. Secondly, this study only observed the changes in short-term postoperative indicators, and the effects of esketamine on patients’ long-term cognitive function and quality of life are still unclear. Future studies need to further extend the follow-up time to comprehensively evaluate its long-term efficacy and safety. In addition, “fragile brain function” is a conceptual framework rather than a reference to a specific metric, we did not develop a new score, this is a research gap. Future investigation could attempt to construct a integrated scoring systems that combine cognitive, imaging, and biological data to better characterize brain vulnerability. Such scores could enhance risk stratification and guide personalized perioperative care.