Using a representative sample of U.S. adults, our analysis identified a significant positive association between AISI and MASLD prevalence, independent of major demographic and clinical confounders. The association remained statistically robust following adjustments for an extensive set of demographic, metabolic, and liver-related variables. These results align with previous studies that implicate systemic inflammation in the development of hepatic steatosis and metabolic liver conditions [30]. Notably, nonlinearity in the association was observed via restricted cubic spline modeling in the AISI–MASLD association, with an inflection point identified at approximately (log _2) AISI = 8.552. Below this threshold, the likelihood of MASLD rose progressively with increasing AISI levels, whereas at higher values, the association plateaued or modestly declined. Such a threshold effect may suggest an underlying immunometabolic mechanism, consistent with the multiple parallel hits hypothesis in MASLD development [21]. Given that AISI integrates several peripheral immune cell counts, our results support its potential utility as a composite marker of systemic inflammation in liver-related epidemiologic research [31].
A growing body of literature has proposed that systemic inflammation plays a central role in the pathophysiology of MASLD, which is echoed by our findings. Numerous prior studies have demonstrated associations between MASLD risk and peripheral blood-based inflammatory indices such as the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and the systemic immune-inflammation index (SII) [25, 28]. For instance, Zhu et al. demonstrated that elevated NLR levels correlated with hepatic steatosis in patients with type 2 diabetes [30], while Kaya et al. reported that both PLR and NLR were associated with the severity of ultrasound-detected MASLD in a Turkish cohort [12]. In the investigation of the associations between MASLD pathogenesis and related indices, BMI represents a critical factor that warrants consideration. Extensive research has established that obesity functions as an independent risk factor for the development of MASLD. The mechanisms underlying this relationship involve the induction of insulin resistance and chronic inflammatory states, both of which contribute to hepatic steatosis and liver injury. Additionally, BMI is inversely correlated with AISI. Metabolic disturbances associated with obesity can interfere with insulin signaling pathways, thereby exacerbating insulin resistance. If not properly adjusted for, obesity can confound the relationship between AISI and MASLD, thereby obscuring their intrinsic association. Therefore, it is essential to account for BMI as an important confounding variable in relevant studies, in order to more accurately elucidate the independent association between AISI and MASLD and to further delineate the pathogenesis of MASLD. In clinical practice, the control of BMI is of critical importance for mitigating the risk of MASLD and improving patient outcomes [4].
In contrast to these more frequently studied indices, the application of AISI in the field of hepatology remains underreported. Most published work to date has focused on its prognostic role in oncology and cardiovascular medicine [32]. Although indicators such as the Neutrophil-to-Lymphocyte Ratio (NLR) and Platelet-to-Lymphocyte Ratio (PLR) have been extensively studied, current research on the AISI is predominantly focused on the fields of oncology and cardiovascular diseases, with relatively limited application in liver-related studies.
The biological plausibility of our findings is underpinned by established immunopathological mechanisms in MASLD. Chronic low-grade inflammation has been recognized as a central driver of hepatic steatosis, insulin resistance, and progressive liver injury, consistent with the multiple parallel hits hypothesis [21]. Neutrophils and monocytes play a pivotal role in hepatic immune responses by producing proinflammatory mediators such as tumor necrosis factor-alpha (TNF-(alpha )), interleukin-6 (IL-6), and reactive oxygen species (ROS). These factors synergistically contribute to hepatocyte damage and oxidative stress, thereby exacerbating liver injury [11].
Platelets actively regulate hepatic microvascular integrity and facilitate leukocyte adhesion and transendothelial migration, thereby amplifying intrahepatic inflammatory cascades [17]. In contrast, lymphopenia—as represented in the denominator of the AISI formula—indicate compromised immune surveillance or immune exhaustion, reflecting an inadequate host response to persistent inflammatory stimuli [18, 22]. Thus, the AISI captures a balance between pro-inflammatory drive and immunoregulatory control. Our study demonstrates that even modest elevations in AISI are linked to higher MASLD prevalence, particularly in individuals without overt comorbidities, supporting its potential role as an early indicator of inflammation-related hepatic dysfunction.
Subgroup analyses revealed that the association between the Aggregate Index of Systemic Inflammation (AISI) and MASLD prevalence was more pronounced among adults aged 20-60 years and individuals without hypertension. This pattern suggests that systemic inflammation may exert a stronger pathogenic role in relatively metabolically healthy populations, wherein traditional cardiometabolic risk factors are less predominant. Conversely, in individuals with established metabolic syndrome or vascular comorbidities, the contribution of systemic inflammation may be attenuated or obscured by multifactorial pathophysiological interactions [19]. From a public health perspective, these results suggest that AISI may be particularly useful for identifying individuals with early-stage or subclinical MASLD who may otherwise go unnoticed in standard metabolic screening algorithms.
The observed nonlinear association between AISI and MASLD prevalence merits further exploration. Restricted cubic spline modeling identified a saturation threshold at (log _2) AISI (approx ) 8.552, beyond which the prevalence of MASLD plateaued and subsequently declined. This attenuation may be attributable to confounding factors [5]. First, elevated AISI levels may be indicative of acute inflammatory conditions, systemic infections, or cancer-associated immune activation. These conditions could introduce confounding effects, thereby obscuring the predictive utility of AISI in the context of chronic hepatic steatosis [32]. Second, the observed attenuation may reflect compensatory immunoregulatory mechanisms. Specifically, the activation of regulatory T cells (Tregs) and the enhanced secretion of anti-inflammatory cytokines, such as interleukin-10 (IL-10), could modulate systemic inflammatory cascades in a threshold-dependent manner. This regulatory response may serve to mitigate hepatic injury, thereby contributing to the observed plateau and subsequent decline in MASLD prevalence [23, 29]. These findings underscore the importance of considering potential nonlinearities and biological ceilings when interpreting inflammatory biomarkers. Future research should aim to further investigate these mechanisms to enhance our understanding of the complex relationship between AISI and MASLD.
In this study, a one-unit increase in (log _2) AISI (i.e., a doubling of AISI) is associated with a 17% increased odds of MASLD (OR = 1.17, 95% CI: 1.08-1.27). To better interpret this finding, we will compare it with effect sizes of other inflammatory markers (e.g., NLR, PLR) and established MASLD risk factors (e.g., BMI, diabetes). For instance, existing research suggests that a one-unit increase in BMI may be linked to a 30% higher risk of MASLD. Compared to such well-known risk factors, the effect size of AISI is relatively small, indicating its predictive capacity for MASLD might be limited. Moreover, we will explore the potential synergistic effects between AISI and other risk factors, and evaluate the added value of AISI in comprehensive risk assessment for MASLD.
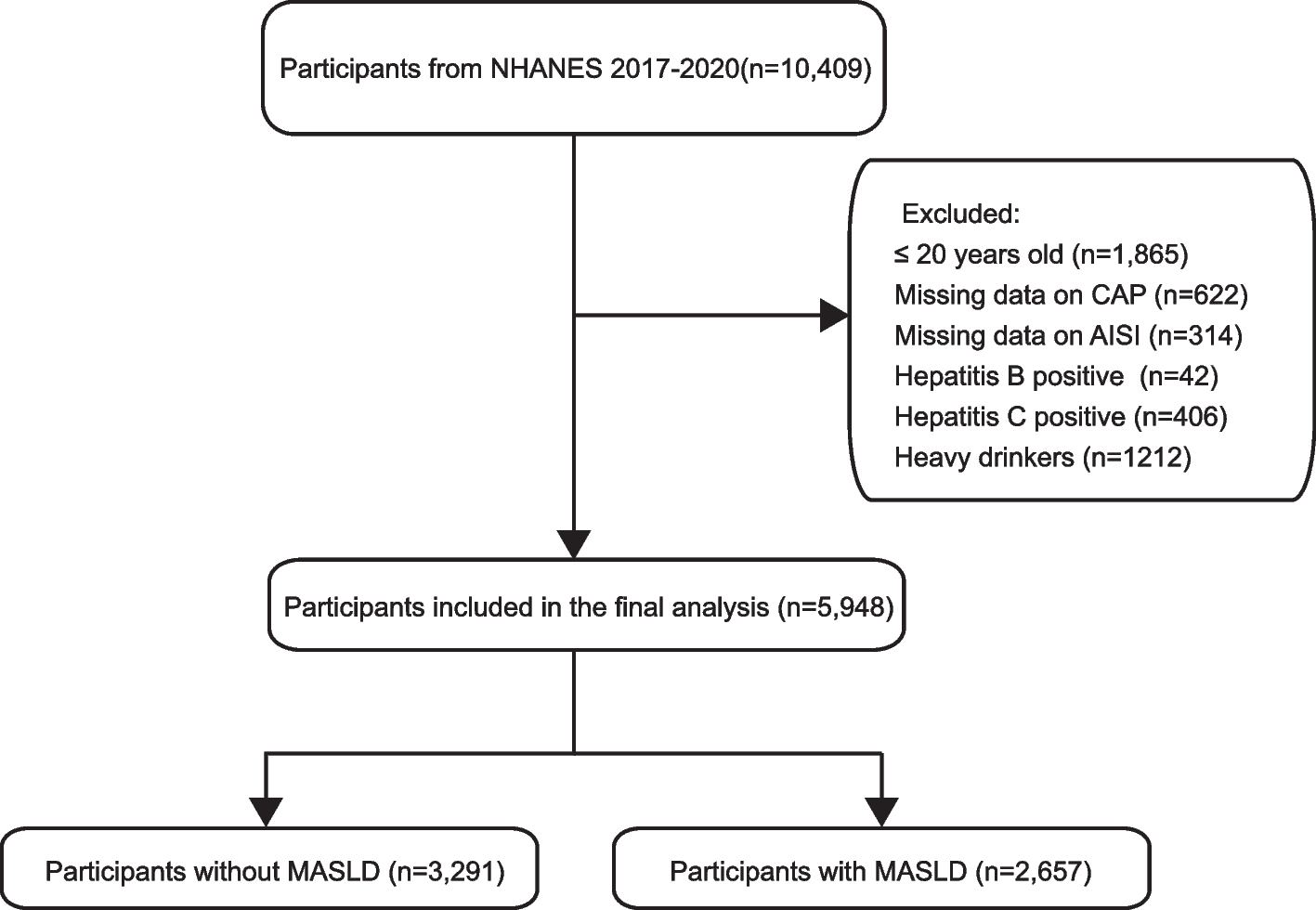
Taken collectively, these results suggest that AISI could serve as a practical, low-cost, and scalable indicator for MASLD risk stratification in routine healthcare settings. As it is derived from standard complete blood count (CBC) parameters, AISI can be easily integrated into everyday clinical workflows, particularly in primary care and community health environments. From a nursing perspective, the use of AISI may enhance early detection efforts, enabling frontline providers to identify individuals at elevated risk and facilitate timely referral for imaging or lifestyle counseling. In contexts where diagnostic infrastructure is limited, AISI may provide an accessible option for population-level liver health screening. However, its modest effect sizes, nonlinear associations, and potential nonspecificity highlight the need for further validation in longitudinal studies before clinical adoption. Nonetheless, this study has several methodological limitations. The cross-sectional design of NHANES inherently limits the ability to infer causality or assess temporal dynamics between inflammation and MASLD onset. Although 43% of the initial sample were excluded due to missing data or predefined criteria, a comparison of baseline characteristics between included and excluded participants (see Appendix Table 7) showed no meaningful differences in age, sex, race/ethnicity, or key metabolic variables, suggesting that selection bias is unlikely to have materially affected our findings. While we controlled for a broad spectrum of demographic and clinical confounders, the possibility of residual confounding from unmeasured lifestyle variables—such as nutrition, physical activity, or pharmacologic exposures—remains.
Additionally, MASLD was identified using transient elastography-derived CAP scores, which, despite their validation, do not offer histopathologic confirmation or fibrosis staging. In this study, we employed CAP (ge )274 dB/m as the diagnostic criterion for MASLD. While CAP is a validated non-invasive method for assessing hepatic steatosis, it has limitations in distinguishing between simple steatosis and NASH or evaluating fibrosis stage, which are critical for MASLD severity assessment. Given that systemic inflammation may be more strongly associated with advanced forms of MASLD such as NASH and significant fibrosis, our inability to stratify by disease severity might have resulted in an underestimation of the association between AISI and severe MASLD [19]. Moreover, the 5% liver fat threshold corresponding to CAP (ge )274 dB/m may include individuals with minimal steatosis who might not have clinically significant MASLD, potentially attenuating the observed association. Future studies should incorporate liver stiffness measurements to assess fibrosis and explore higher CAP thresholds in sensitivity analyses. This would enhance the understanding of the relationship between systemic inflammation and MASLD across different disease stages [6]. Our findings provide a foundation for further research into AISI as a potential screening tool for MASLD risk in general populations and underscore the need for additional studies to clarify its clinical utility.A further limitation is that AISI may be influenced by transient inflammatory responses unrelated to liver disease, potentially diminishing its specificity. Furthermore, the calculation of AISI involves multiple laboratory measurements, each with inherent measurement error. The propagation of these errors through the AISI formula could introduce substantial variability that is not accounted for in the analysis. Future analyses should consider these limitations and conduct sensitivity analyses excluding participants with evidence of acute inflammation, such as elevated C-reactive protein or white blood cell count.
Future studies employing longitudinal designs and interventional methodologies are needed to clarify the temporal role of AISI in MASLD development and to assess its predictive value in tracking disease progression or response to targeted interventions.