Cesarean section between June 2024 and October 2024 in the Department of Perinatology, Health Sciences University, Etlik City Hospital, Ankara, Türkiye were prospectively included in the study.
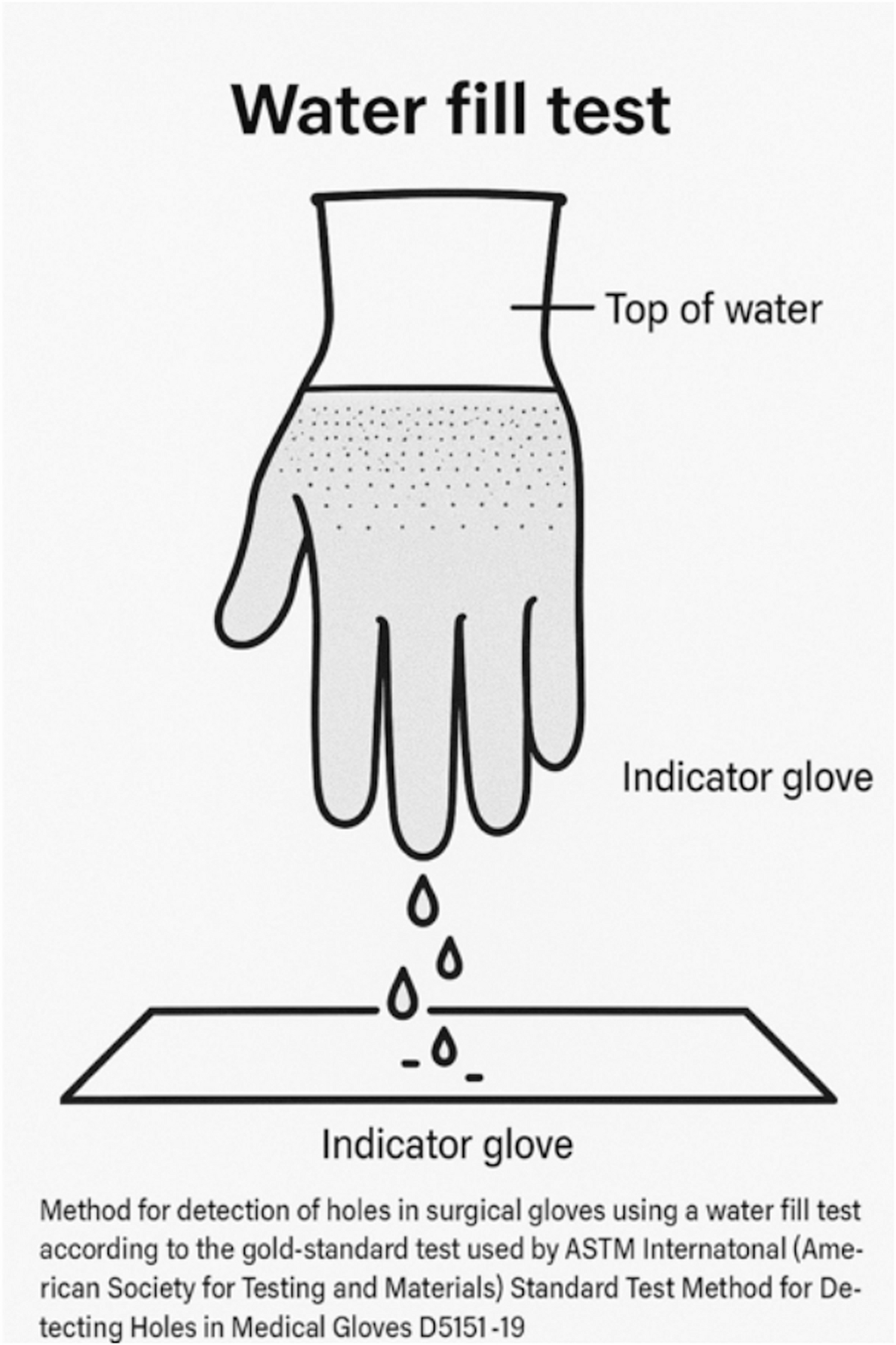
The surgical teams consisted of an experienced specialist in obstetrics and gynecology (more than four years after graduation), a senior resident and a surgical nurse with at least four years of experience in assisting with cesarean sections. All surgical operations performed by the specialist. Operating room staff and surgeons were informed and trained on the collection procedures. Plastic baskets were placed in each operating room and the team members placed the used gloves in these baskets after the each operation. All used surgical gloves from the scrubbed surgical team were collected. Collected gloves were inspected visually for macro perforation just after placing in the basket. Patients were excluded from the study if any glove used by the scrubbed surgical team showed a macro-perforation either noticed intraoperatively or identified during immediate visual inspection after the surgery. The remaining gloves, which appeared visually intact, were examined using a water-fill test, right after the each surgery, in the concurrent operation room, during the operation room cleaning, according to the American Society for Testing and Materials [6]. Under standard operation room temperature, a 38 cm long plastic tube was used for the test. The gloves were attached to the distal end of the tube and 1000 ml of tap water was poured through the tube into the gloves. The perforation was recognized as water leakage or water jet from the glove surface or as droplet formation at the toe tip. The observation time was two minutes. Gloves with a positive water filling test were defined as the study group and negative gloves as the control group (Figs. 1 and 2).
Water Fill Test Method for Detecting Glove Perforations

Glove Perforation Demonstrated by Water Fill Test in a Clinical Setting
Elective cesarean deliveries were defined as planned procedures performed before the onset of labor in clinically stable patients, whereas emergency cesarean deliveries included all other cases, including those with labor or clinical indications such as prolonged rupture of membranes, maternal fever, or fetal distress. Patients who were categorized as class 1 or 2 according to the American Society of Anesthesiologists (ASA) physical status classification were included in the study. The surgical site was cleaned by senior resident, with alcohol and combined with 4% chlorhexidine and waited some minutes for air-dried. The urinary catheter was placed preoperatively in the operating room. After skin antisepsis and urinary catheterization, the surgical area was draped using sterile, disposable surgical drape sets. Draping was performed by the senior resident in accordance with standard sterile technique protocols. Pfannenstiel skin incision, incision in the lower segment of the uterus, detachment of the placenta by fundal massage, exteriorization of the uterus for repair, single-layer uterine closure, suture closure of the subcutaneous layer if the subcutaneous tissue was thicker than 2 cm, subcutaneous closure with a Prolene suture, and the use of a blunt needle tip were established as standard surgical procedures in the study. Antibiotic prophylaxis (2 g cephazolin) was administered intravenously before skin incision. Single layer latex gloves were used for all procedures and double-gloved surgeries did not included to study. Early removal of the urinary catheter was performed routinely. Patients were physically examined daily during hospitalization and again in person on postoperative days 10 and 30 by the attending obstetrician.
The diagnosis of surgical site infection, diagnosed by specialist in obstetrics and gynecology, was based on the definition of the National Healthcare Safety Network of the United States Centers for Disease Control and Prevention [7]. Superficial surgical site infections were analyzed for the study. Deep incisions or organ/space infections did not occur in the study groups.
Subjects were excluded if they: (1) did not provide informed consent, (2) had a history of inflammatory disease or clinical chorioamnionitis, (3) had multiple pregnancies, (4) were classified as ASA class III or higher, (5) underwent midline skin incision, (6) had known allergies to chlorhexidine, antibiotics, or latex, or (7) were lost to follow-up.
All patients gave their informed consent to participate in this project. The study was approved by the institution’s ethics committee and was conducted in accordance with the Declaration of Helsinki.
Sample size
A priori sample size calculation was performed using G*Power version 3.1.9.7. In the absence of previous studies to estimate the effect size, a medium effect size (w = 0.3) was assumed. With α = 0.05 and power = 0.80, the required sample size for a chi-square test with 1 degree of freedom was calculated as 88 participants (44 per group). However, due to the naturally occurring frequency of glove perforation during the study period, only 32 patients could be included in the perforation group. The control group included 505 patients, reflecting the actual surgical population.
To evaluate the adequacy of this sample, a post-hoc power analysis was also conducted based on the observed effect size (w = 1.545). With α = 0.05 and a total sample size of 537 (n₁ = 505, n₂ = 32), the calculated power (1 − β) exceeded 99.9%, indicating sufficient statistical sensitivity to detect differences between groups.
Statistical analysis
All statistical analyses were performed using Jamovi version 2.6.26 (The Jamovi Project, Sydney, Australia). The variables were examined using visual (histogram, probability plots) and analytical methods (Kolmogrov-Simirnov/Shapiro-Wilk test) to determine whether they were normally distributed or not. The Levene test was used to assess the homogeneity of variance. Descriptive analyzes using medians and interquartile ranges (IQR) (Q1-Q3) were performed for the non-normally distributed numerical data. Mann-Whitney U-tests were performed to compare these parameters between the groups. For the categorical variables, descriptive analyzes were performed using frequencies and percentages. The relationships between the categorical variables were analyzed using the chi-square test or Fisher’s exact test. A p-value of less than 0.05 was considered a statistically significant.
Additionally, a multivariable logistic regression analysis was performed to evaluate the independent association between glove micro-perforation and surgical site infection (SSI). Known confounding variables including emergency cesarean section, diabetes mellitus, obesity, surgical duration, and intraoperative blood loss were included in the model to adjust for potential effects.