The global burden of strokes
Between 1990 and 2021, the global burden of stroke in women of reproductive age generally declined. Specifically, the prevalence of ischemic stroke increased, the YLDs rate remained stable, and the DALYs rate increased. In contrast, the burden of ICH and SAH showed an overall downward trend (Supplementary Fig. 1 and 2).
In 2021, the prevalence of stroke was 527.51 (95%UI: 486.94 to 564.65), with an AAPC of −0.22 (95%CI: −0.23 to −0.21). The YLDs rate was 83.89 (95%UI: 59.70 to 107.25), with an AAPC of −0.33 (95%CI: −0.37 to −0.30), and the DALYs rate was 432.28 (95%UI: 392.06 to 472.61), with an AAPC of −1.27 (95%CI: −1.30 to −1.23) (see Table 1).
For ischemic stroke, the prevalence rate was 330.12 (95%UI: 294.61–364.87), with an AAPC of 0.08 (95%CI: 0.07 to 0.09). The YLDs rate was 51.79 (95%UI: 36.79 to 67.04), with an AAPC of 0.00 (95%CI: −0.02 to 0.03), and the DALYs rate was 103.77 (95%UI: 86.24 to 121.68), with an AAPC of −0.49 (95%CI: −0.52 to −0.45) (see Supplementary Table 1).
For ICH, the prevalence rate was 128.83 (95%UI: 115.55 to 143.89), with an AAPC of −0.83 (95%CI: −0.86 to −0.81). The YLDs rate was 21.00 (95%UI: 14.84 to 27.98), with an AAPC of −0.93 (95%CI: −0.99 to −0.85), and the DALYs rate was 258.64 (95%UI: 228.30 to 286.74), with an AAPC of −1.37 (95%CI: −1.42 to −1.33) (see Supplementary Table 2).
For SAH, the prevalence rate was 69.60 (95%UI: 62.39 to 78.02), with an AAPC of −0.41 (95%CI: −0.47 to −0.38). The YLDs rate was 11.09 (95%UI: 7.65 to 14.46), with an AAPC of −0.53 (95%CI: −0.59 to −0.47), and the DALYs rate was 69.86 (95%UI: 62.26 to 82.45), with an AAPC of −1.86 (95%CI: −1.89 to −1.83) (see Supplementary Table 3).
Global trends by regions
From 1990 to 2021, the stroke burden in women of reproductive age across the five SDI regions generally exhibited a declining trend. However, significant regional variations in stroke and related indicators were observed in 2021. Overall, the burden of stroke was the highest in the High-middle SDI regions and the lowest in the Low SDI regions, with the latter showing a pronounced decrease. Among the different stroke subtypes, ischemic stroke presented the highest burden in the High-middle SDI regions, whereas the most notable reductions in burden were observed for ICH and SAH in the Low SDI regions. The stroke-related DALYs rates across all SDI regions displayed a downward trend, with the High–middle SDI regions showing the most substantial reduction. Notably, the Low SDI regions experienced the most marked decrease in both prevalence and YLDs rates for ischemic stroke, whereas the other regions exhibited a general upward trend (see Supplementary Fig. 1 and Supplementary Fig. 2).
In 2021, stroke indicators showed significant disparities between different SDI regions. The prevalence of stroke was highest in High-middle SDI regions (580.59, 95%UI: 532.15 to 624.36) and lowest in Low SDI regions (467.34, 95%UI: 438.79 to 497.32), with a notable downward trend observed in Low SDI regions (AAPC: −0.45, 95%CI: −0.46 to −0.45). The YLDs rate peaked in the High-middle SDI regions (106.57, 95%UI: 74.27 to 136.43) and was at its lowest in the Low SDI regions (63.82, 95UI: 46.04 to 81.09), with the most pronounced decline in the Low SDI regions (AAPC: −0.45, 95%CI: −0.50 to −0.42). The DALYs rate was highest in the Low-middle SDI regions (500.18, 95%UI: 446.86 to 559.40) and lowest in the High SDI regions (221.88, 95%UI: 199.22 to 246.92), with the most notable reduction occurring in High SDI regions (AAPC: −1.61, 95%CI: −1.63 to −1.57) (see Table 1).
Please refer to the Supplementary Materials and Table 1 for detailed results on the burden of stroke subtypes across the five SDI and global regions.
Supplementary Fig. 3 illustrates the distribution of prevalence, YLDs, and DALYs rates for ischemic stroke, ICH, and SAH across the 27 super-regions. In these regions, ischemic stroke accounted for the largest proportion of both the prevalence and YLDs rates. ICH contributed to the highest proportion of DALYs rates across most regions, highlighting a distinct trend from other stroke indicators.
Global trends by countries and SDI
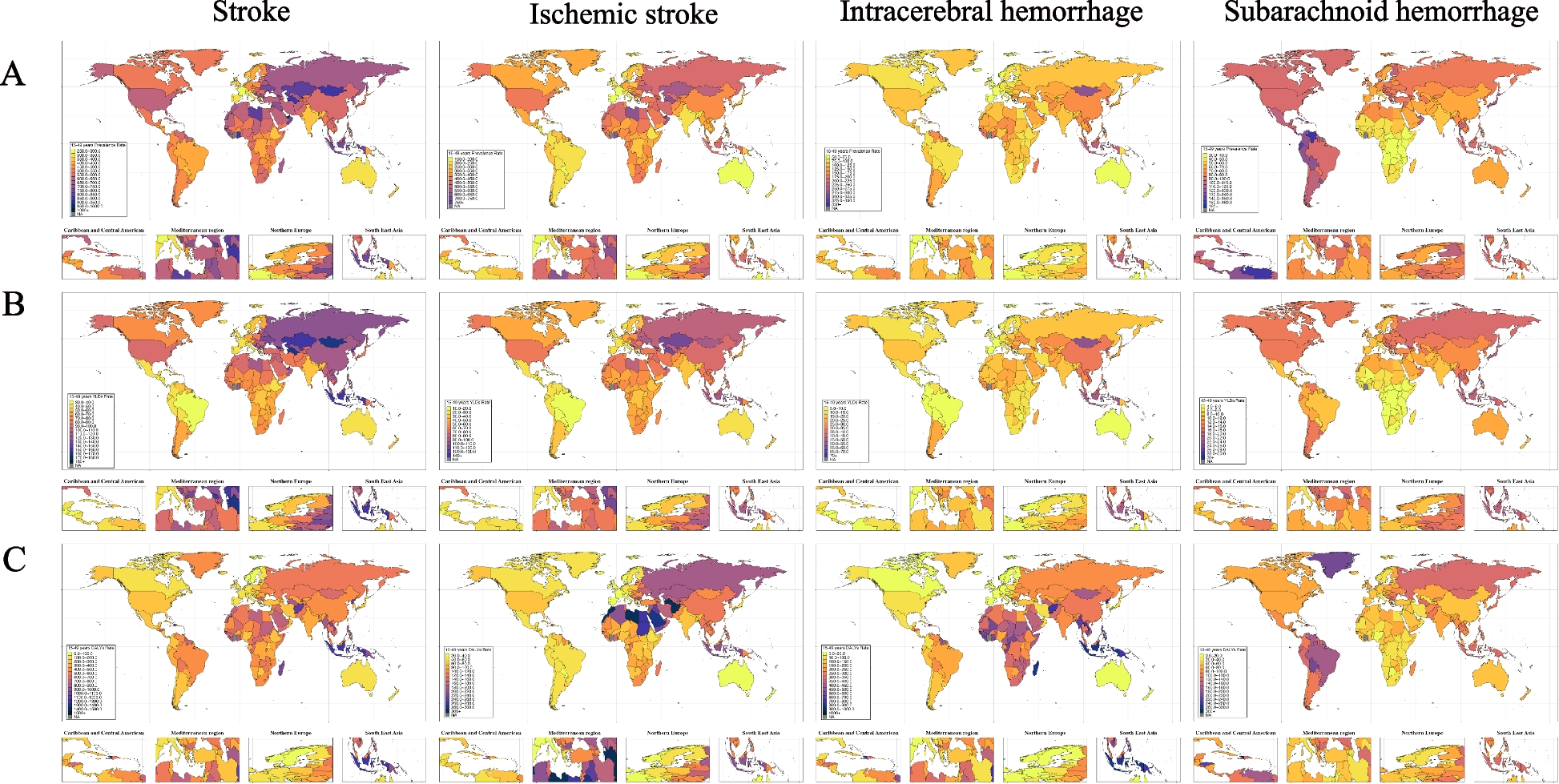
We conducted an analysis of the burden of stroke, ischemic stroke, ICH, and SAH, focusing on prevalence, YLDs, and DALYs rates across 204 countries and regions globally in 2021 (see Fig. 1).
The burden of prevalence, YLDs, and DALYs rate of stroke, ischemic stroke, ICH, and SAH among women of reproductive age in 204 countries and territories worldwide in 2021. A The burden of prevalence rate of stroke, ischemic stroke, ICH, and SAH among women of reproductive age in 204 countries and territories worldwide in 2021. B The burden of YLDs rate of stroke, ischemic stroke, ICH, and SAH among women of reproductive age in 204 countries and territories worldwide in 2021. C The burden of DALYs rate of stroke, ischemic stroke, ICH, and SAH among women of reproductive age in 204 countries and territories worldwide in 2021
In 2021, we observed considerable regional variations in stroke burden indicators. Nauru had the highest prevalence, YLDs, and DALYs rates, with values of 1,223.56 (95% UI: 1,180.50 to 1,271.92), 241.44 (95% UI: 173.40 to 311.30), and 2,646.68 (95% UI: 1,977.34 to 3,663.05), respectively. Conversely, Switzerland exhibited the lowest prevalence and DALYs rates, at 287.78 (95% UI: 267.64–308.64) and 70.69 (95% UI: 57.65 to 83.30), respectively. Paraguay, on the other hand, had the lowest YLDs rate of 33.11 (95% UI: 23.89 to 43.01) (see Supplementary Table 4).
Please refer to Supplementary Materials for detailed results on the burden of stroke subtypes across 204 countries and territories.
We also explored the relationship between the SDI values and stroke burden indicators in 204 countries and regions from 1990 to 2021. These findings revealed that the burden of ischemic stroke and ICH generally decreased over time as well as with increasing SDI values. The burden of SAH exhibited a gradual increase with time and SDI values until it reached an SDI value of approximately 0.60, at which point it peaked. Following this peak, the burden began to decline as both the time and SDI values continued to increase (see Fig. 2).
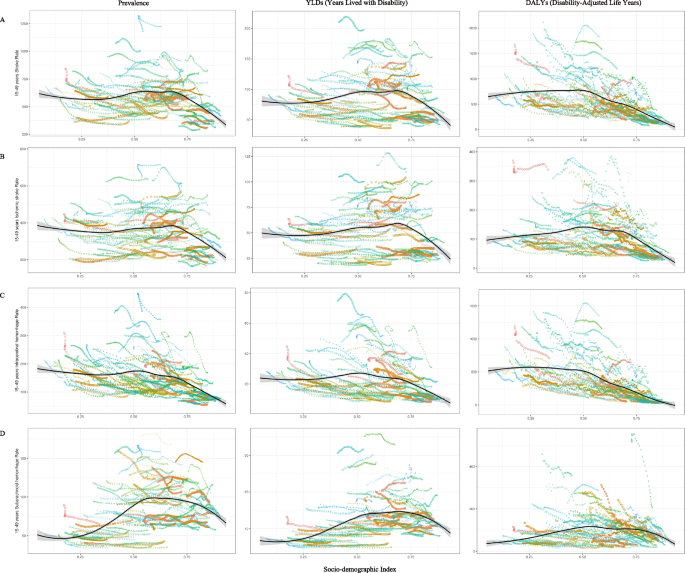
The trends in the burden of stroke, ischemic stroke, ICH, and SAH in terms of prevalence, YLDs, and DALYs rates among women of reproductive age across 204 countries and regions globally from 1990 to 2021, based on SDI values. A The trends in the burden of stroke in terms of prevalence, YLDs, and DALYs rates among women of reproductive age across 204 countries and regions globally from 1990 to 2021, based on SDI values. B The trends in the burden of ischemic stroke in terms of prevalence, YLDs, and DALYs rates among women of reproductive age across 204 countries and regions globally from 1990 to 2021, based on SDI values. C The trends in the burden of ICH in terms of prevalence, YLDs, and DALYs rates among women of reproductive age across 204 countries and regions globally from 1990 to 2021, based on SDI values. D The trends in the burden of SAH in terms of prevalence, YLDs, and DALYs rates among women of reproductive age across 204 countries and regions globally from 1990 to 2021, based on SDI values
Variation in stroke burden across different age groups
Comprehensive age-specific burden estimates for stroke and its subtypes are presented in Supplementary Materials. From 1990 to 2021, the overall burden of stroke in women of reproductive age has shown a clear downward trend. More specifically, the burden of ischemic stroke, ICH, and SAH demonstrated declines across various indicators, with the most pronounced reductions occurring in the DALYs rates (see Supplementary Fig. 4).
The 15–24 age group experienced the most substantial reduction in stroke prevalence, with an AAPC of −0.59 (95%CI: −0.61 to −0.58). The 20–24 age group showed the most significant decline in the YLDs rate, with an AAPC of −0.87 (95%CI: −0.91 to −0.83). The 35–39 age group demonstrated the largest reduction in the DALYs rate, with an AAPC of −1.82 (95%CI: −1.85 to −1.79) (see Table 1).
For ischemic stroke, the 20–24 age group showed the most notable decrease in both prevalence and YLDs rates, with AAPCs of −0.34 (95%CI: −0.36 to −0.33) and −0.57 (95%CI: −0.63 to −0.52), respectively. In comparison, the 45–49 age group exhibited the most significant decline in DALYs rate, with an AAPC of −1.03 (95%CI: −1.06 to −0.99) (see Supplementary Table 1).
In the analysis of ICH, the 45–49 age group had the most substantial decrease in prevalence rate, with an AAPC of −1.31 (95%CI: −1.35 to −1.29), while the 20–24 age group showed the greatest reduction in YLDs rate, with an AAPC of −1.44 (95%CI: −1.56 to −1.32). The 35–39 age group showed the most significant drop in DALYs rate, with an AAPC of −2.00 (95%CI: −2.03 to −1.97) (see Supplementary Table 2).
For SAH, the 45–49 age group displayed the most pronounced decrease in prevalence rate, with an AAPC of −0.82 (95%CI: −0.84 to −0.81), while the 20–24 age group experienced the largest reduction in YLDs rate, with an AAPC of −1.06 (95%CI: −1.20 to −0.88). The 35–39 age group showed the most significant drop in the DALYs rate, with an AAPC of −2.35 (95%CI: −2.40 to −2.31) (see Supplementary Table 3).
We found that, as age increased, the burden of various types of strokes also tended to increase. Among all stroke types, ischemic stroke exhibited the highest prevalence and YLDs rates in the same age group in 1990 and 2021, whereas SAH had the lowest prevalence and YLDs rates. Intriguingly, ICH consistently had the highest DALYs rate in the same age group across the same period, highlighting a distinct trend compared with the prevalence and YLDs rates (see Fig. 3).
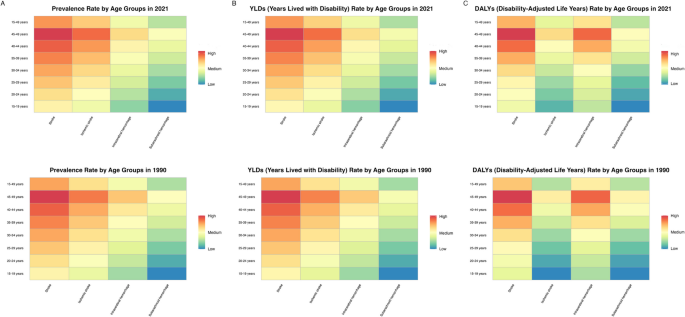
The burden of stroke, ischemic stroke, ICH, and SAH in terms of prevalence, YLDs, and DALYs among women of reproductive age across different age groups globally in 1990 and 2021. A The burden of stroke, ischemic stroke, ICH, and SAH in terms of prevalence rate among women of reproductive age across different age groups globally in 1990 and 2021. B The burden of stroke, ischemic stroke, ICH, and SAH in terms of YLDs rate among women of reproductive age across different age groups globally in 1990 and 2021. C The burden of stroke, ischemic stroke, ICH, and SAH in terms of DALYs rate among women of reproductive age across different age groups globally in 1990 and 2021
Strokes-related DALYs rate in different regions and age groups associated with risk factors
In 2021, 23 risk factors were related to the DALY rates of stroke and ischemic stroke, 17 risk factors were associated with the DALY rates of ICH, and 14 risk factors were linked to the DALY rates of SAH (see Fig. 4). As age increased, the association between these risk factors and the DALY rates of stroke and its subtypes became progressively more pronounced, and the number of relevant risk factors also increased (see Fig. 4).
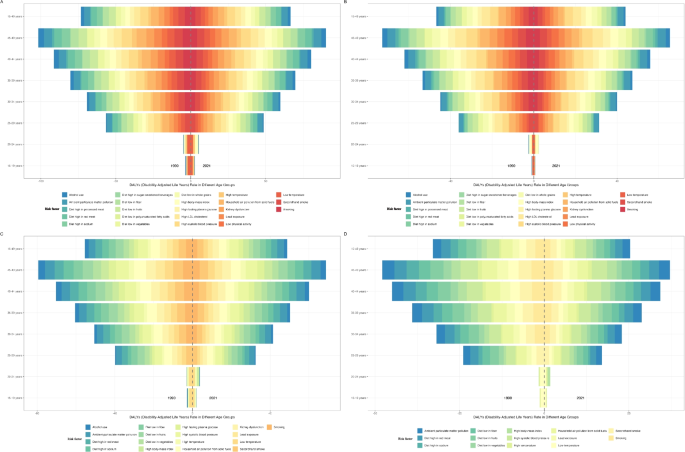
The DALYs rates related to stroke, ischemic stroke, ICH, and SAH associated with risk factors among women of reproductive age in different age groups globally in 2021. A The DALYs rates related to stroke associated with risk factors among women of reproductive age in different age groups globally in 2021. B The DALYs rates related to ischemic stroke associated with risk factors among women of reproductive age in different age groups globally in 2021. C The DALYs rates related to ICH associated with risk factors among women of reproductive age in different age groups globally in 2021. D The DALYs rates related to SAH associated with risk factors among women of reproductive age in different age groups globally in 2021
Risk factors affecting stroke-related DALYs rates in women of reproductive age can be categorized into three main types: metabolic, environmental/occupational, and behavioral risks. Compared with 1990, among the three categories of risk factors, stroke-related DALYs associated with metabolic risks exhibited a continued upward trend, whereas those associated with environmental/occupational and behavioral risks showed a declining trajectory across 27 super-regions. This trend was also evident in the DALYs related to ischemic stroke, ICH, and SAH (Fig. 5).
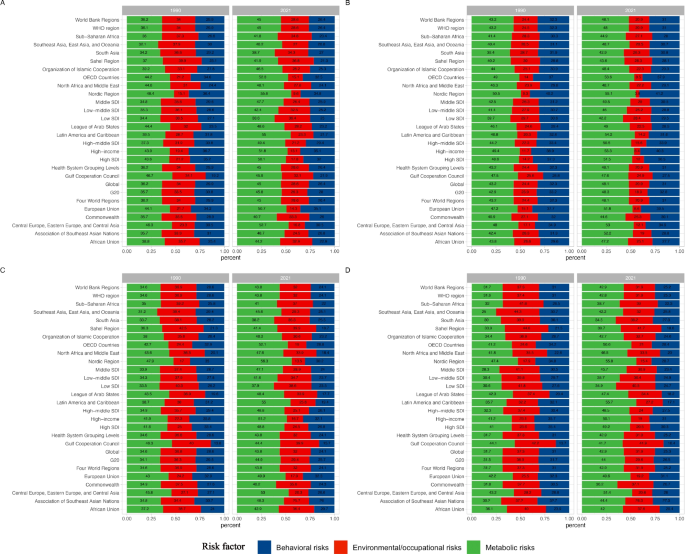
The DALY rates related to stroke, ischemic stroke, ICH, and SAH associated with metabolic, environmental/occupational, and behavioral risk factors in the 27 GBD super-regions worldwide in 1990 and 2021. A The DALY rates related to stroke associated with metabolic, environmental/occupational, and behavioral risk factors in the 27 GBD super-regions worldwide in 1990 and 2021. B The DALY rates related to ischemic stroke associated with metabolic, environmental/occupational, and behavioral risk factors in the 27 GBD super-regions worldwide in 1990 and 2021. C The DALY rates related to ICH associated with metabolic, environmental/occupational, and behavioral risk factors in the 27 GBD super-regions worldwide in 1990 and 2021. D The DALY rates related to SAH associated with metabolic, environmental/occupational, and behavioral risk factors in the 27 GBD super-regions worldwide in 1990 and 2021
We analyzed the risk factors associated with stroke-related DALY rates in women of reproductive age from 1990 to 2021, along with trends in their attributable burden. The analysis revealed a significant upward trend in DALY rates linked to four specific risk factors over the period: “Diet high in sugar-sweetened beverages” (AAPC = 2.33), “High body-mass index”(AAPC = 1.81), “High temperature” (AAPC = 0.77), and “High fasting plasma glucose” (AAPC = 0.51). However, “ambient particulate matter pollution” did not have a statistically significant effect on the DALY rate. Seventeen other risk factors showed downward trends. Because of the inability of the Joinpoint software to handle negative values, analysis of the impact of “diet high in red meat” on the DALY rate was not conducted in this study (see Supplementary Table 5).
In women of reproductive age, “high systolic blood pressure” demonstrated the strongest association with DALY rates among all assessed risk factors for stroke, ICH, and SAH, with contributions of 177.67 (95% UI: 120.80 to 234.60), 108.93 (95% UI: 75.44 to 146.96), and 26.97 (95% UI: 18.16 to 36.75), respectively. “Diet high in red meat” was associated with the lowest stroke burden, with values of −28.66 (95% UI: −121.24 to 36.86), −21.56 (95% UI: −88.88 to 27.57), and −7.77 (95% UI: −32.18 to 9.97). “High LDL cholesterol” demonstrated the strongest association with DALY rates of ischemic stroke, with an estimated value of 51.58 (95% UI: 25.68 to 73.64), whereas”diet low in polyunsaturated fatty acids”was associated with the lowest stroke burden, with a value of 0.05 (95% UI: 0.02 to 0.08) (see Supplementary Table 6).
Similar patterns were observed in the 45–49 age group. The DALY rates for stroke, ICH, and SAH were strongly correlated with”high systolic blood pressure,”with values of 665.65 (95% UI: 882.12–465.50), 427.90 (95% UI: 573.32–301.72), and 87.78 (95% UI: 118.37 to 59.28), respectively.”Diet high in red meat”was associated with a relatively minor association, with values of −76.82 (95% UI: 103.01 to −327.12), −61.77 (95% UI: 80.40 to −262.75), and −17.20 (95% UI: 23.48 to −70.54).”High LDL cholesterol”exhibited the strongest association with the burden of ischemic stroke–related DALYs, at 154.88 (95% UI: 74.22 to 221.02).
We observed substantial uncertainty in the DALY rates of different stroke subtypes associated with several risk factors, including the”diet high in red meat,””diet low in whole grains,””diet low in fiber,”and”lead exposure”. The 95% UI for these risk factors encompassed zero, indicating that their effect on stroke DALY rates was ambiguous and likely lacked statistical significance.