Study design, area, period and population
The study was conducted at Tamale Teaching Hospital (TTH) in the Northern Region of Ghana. TTH is the primary referral hospital in the five Northern regions of the country and was established in 1974. The hospital has a bed capacity of around 800 and provides specialist services in various fields, including obstetrics and gynaecology, surgery, orthopaedics and trauma, internal medicine, child health, pathology, ear, nose and throat, opthalmology, endoscopy, neurosurgery, anaesthesia and intensive care, psychiatry, dentistry, pharmacy, laboratory, and outpatient department. On the average, the hospital conducts about 8,000 deliveries annually. In this retrospective cross-sectional study, the birth records of all women who delivered live babies at TTH between October and December 2021 were reviewed.
Study variables
Outcome variable
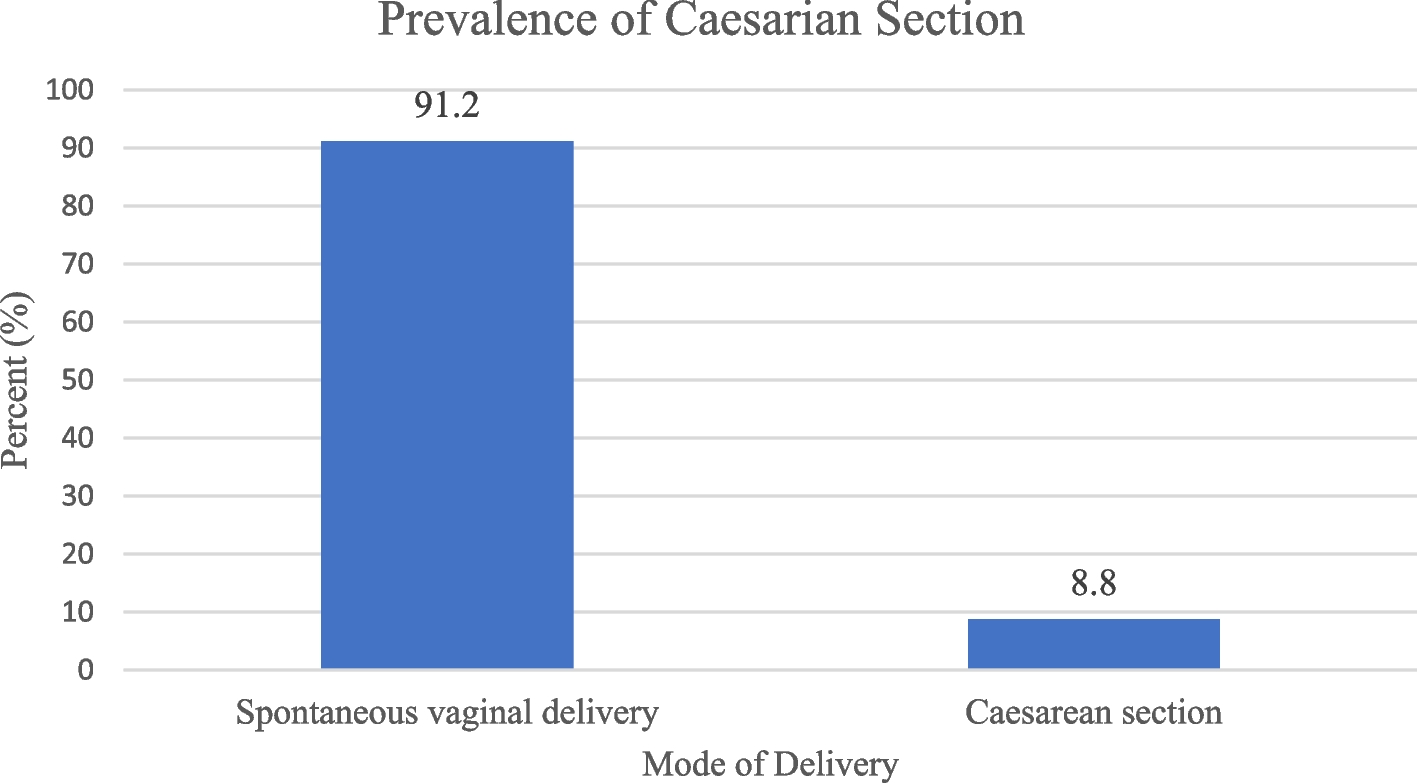
The dependent variable was caesarean delivery. Delivery was dichotomised into “Spontaneous vaginal delivery” when mother delivered through the vagina and “caesarean delivery” when mother delivered through caesarean section. Birth records that documented all the types of caesarean delivery (planned/elective and emergency) were included.
Dependent variable
The main predictors included obstetric characteristics such as type of birth (singleton or multiple), gravidity, parity, gestational age, number of pregnancies in the last five years, previous history of low birth weight (LBW), abortion, stillbirth, and any obstetric complications. Additional predictors included family history of hypertension and the use of long-lasting insecticidal nets (LLINs), which were included due to their relevance to maternal health status. Low birth weight (LBW) is defined as a birth weight of less than 2,500 g (2.5 kg) at birth [25]. Sulfadoxine-Pyrimethamine (SP) doses were categorized as standard and non-standard: the standard dose involves two doses of SP administered during the second and third trimesters for intermittent preventive treatment of malaria, while non-standard doses refer to deviations from this regimen, such as fewer or more doses or doses given outside the recommended timing. In terms of antenatal care (ANC), timely ANC visits were defined as the first visit occurring before 16 weeks of gestation [26], while delayed ANC visits referred to the first visit occurring after 16 weeks. Furthermore, recommended ANC visits referred the mother who had at least four ANC visits, as per the World Health Organization (WHO) guidelines [26], with any fewer visits categorized as not recommended. Additionally, maternal conditions such as Hepatitis B, hypertension, anemia, sickling status, HIV, malaria, and other infections or conditions were also considered. Hypertension was classified as absent when blood pressure was ≤ 120/80 mmHg and present when blood pressure was ≥ 140/90 mmHg, while anemia was defined as a haemoglobin level of < 11.0 g/dl, with normal levels being ≥ 11.0 g/dl. These factors were critical in understanding the predictors of maternal and pregnancy outcomes in the study population.
Data on maternal conditions were extracted from routine tests conducted on pregnant women during their antenatal care visits. Maternal conditions, including Hepatitis B, pre-eclampsia, hypertension during antenatal care, haemoglobin levels at registration and 36 weeks, sickling status, HIV status, malaria infection during pregnancy, syphilis infection during pregnancy, and hypertension prior to pregnancy, were documented and monitored throughout the course of antenatal care.
Inclusion
The study included birth records of mothers who delivered live babies after the gestational age of viability (≥ 28 weeks) at Tamale Teaching Hospital between October and December 2021. As a retrospective cross-sectional study, data were extracted from hospital records. Therefore, direct consent from the mothers was not sought; however, ethical clearance and institutional permission were obtained to ensure the use of anonymized patient data for research purposes.
Exclusion criteria
Mothers who underwent laparotomy for extra-uterine pregnancy and those who had non-live births following caesarean section were excluded from this study. This criterion was applied to focus on the outcomes of live births, which are the primary interest of this study in examining maternal and neonatal health outcomes following caesarean section. Non-live births, such as stillbirths or other pregnancy losses, were excluded as they could introduce additional confounding factors that are outside the scope of this study’s objective of assessing maternal health outcomes and delivery mode preferences in live birth deliveries.
Data extraction and sample size
A pretested data extraction sheet was used to obtain information on maternal demographics, obstetric history, ANC attendance, delivery details, and neonatal outcomes. Additionally, to complement missing or incomplete information in the hospital records, particularly on socio-demographic characteristics and maternal preferences, follow-up interviews were conducted with a subset of mothers at their homes in Tamale township.
Trained research assistants, basically midwives, were oriented on the eligibility criteria for inclusion in the study and the data extraction process. Data collection was supervised daily to ensure consistency, completeness, and accuracy of the extracted data. During the study period, a total of 598 live births were recorded. However, 36 records were excluded due to laparotomies for extra-uterine pregnancies and incomplete birth records. As a result, 318 cases were included in the final analysis, representing approximately 56.2% of all live births during the study period.
Data management and analysis
Before data entry, data extraction sheets and semi-structued questionnaires were subjected to accuracy checks. The Kobo Collect app was used for data entry, and the data was exported to STATA version 17 for analysis. Descriptive statistics were used to calculate frequencies and percentages were reported for categorical variables. For continuous variables, means and standard deviations were determined. To determine the mother’s economic status, various socioeconomic indicator variables were considered, such as the mother’s and father’s profession and education, type of housing, water supply, presence of an indoor kitchen, electricity, indoor toilet, fridge, car, motorcycle, bicycle, and membership in health insurance.
All socioeconomic information was self-reported by the mothers, and no direct observations were made during the interviews. Principal component analysis (PCA) was used on the relevant socioeconomic indicator variables that contributed to a combined socioeconomic status score factor of more than 10%. The SES of each household was described using the first principal component (i.e., the component with the highest eigenvalue), which reflects the greatest variation in asset ownership (wealth index). The factor scores generated were then divided into terciles to classify households into the following categories: 33% of households were classified as low, and the highest 33% were classified as having high socioeconomic status.
Univariate logistic regression analysis was used to identify associations between variables and Caesarean section (Model I), followed by a stepwise multivariate logistic regression model (Model II) that considered variables that were significant in the univariate logistic regression. The goodness of fit of Model II was examined using the likelihood ratio test by comparing the likelihood of the data under the full and alternative models. If the overall model recorded a p-value less than 0.05, the model was considered good. The variable inflation factor (VIF) was used to cater to multicollinearity, and explanatory variables with VIF values exceeding 5 were excluded from Model II. Adjusted odds ratios and confidence intervals were computed with p values < 0.05 and were considered statistically significant in Model II.
Ethical considerations
Ethical approval for this study was obtained from the Department of Research and Development, Tamale Teaching Hospital. The ethical clearance number for this study is TTH/R&D/SR/152. Informed consent was obtained from the respondents before conducting the interviews. The data obtained from the study was kept confidential, and personal information was anonymised during the data collection, analysis, and dissemination of findings. Identification codes were used for data management, storage, analysis, and reporting. A file containing information about the participants was stored in a cabinet and kept under lock. The file was accessible only to the principal investigator.