Pertussis is a highly contagious respiratory infection worldwide, experiencing epidemic spikes every 2–5 years and affecting individuals across all age groups [12]. It is particularly devastating for infants who suffer from the highest age-specific incidence and are responsible for nearly all pertussis hospital admissions and fatalities [13]. This may be due to the lack of vaccination during the first three months of life and the insufficient titer of maternally transmitted antibodies for effective protection. The most frequent complications of pertussis include pulmonary, neurologic, and nutritional [14]. A prospective multicenter surveillance study in Germany showed that the overall rate of major complications in infants and children with pertussis was 6% [15]. In severe cases, children would die from respiratory failure or acute pertussis encephalopathy. Son et al. conducted a multinational survey among Asian children and adolescents and found evidence of substantial B. pertussis circulation, indicating that 1 in 20 individuals has recently been infected, irrespective of their vaccination status [16]. Early discovery, diagnosis and treatment were essential to reduce disease severity and duration of pertussis, thereby improving patients’ quality of life.
Currently, the diagnosis of pertussis encompasses both clinical and laboratory assessments. However, the reduction in typical pertussis cases post-vaccination has made early detection challenging for clinicians using current clinical case definitions, often resulting in undiagnosed or misdiagnosed cases. Laboratory diagnostic methods include pathogen isolation, nucleic acid amplification tests, and detection of specific antibodies in serum. This is particularly crucial for cases of pertussis presenting with atypical symptoms, as laboratory testing serves as a vital tool for accurate disease diagnosis. Culturing and isolating the B. pertussis remains the gold standard for diagnosing pertussis with significant limitations. As a fastidious bacterium, B. pertussis requires special culture media and conditions, and its slow growth rate making culture time-consuming and unable to meet the need for early diagnosis and treatment in clinical practice [17]. The serological antibody detection also faces limitations, primarily due to the time constraints. Antibodies may not be detectable in patients until after a certain incubation period following exposure to the antigen. Additionally, vaccination against pertussis can lead to increased antibody levels, complicating the interpretation of test results [18]. PCR detection has emerged as the preferred method for diagnosing pertussis internationally, offering a short turnaround time, high sensitivity, and a low risk of contamination [19]. However, this method requires specialized laboratory equipment and technical expertise, which can be challenging to access in resource-limited settings and is relatively expensive.
To address this, we developed a predictive model for pertussis in children which can reliably assist clinicians in diagnosing pertussis. Timely management of patients predicted to be positive through our model could play a crucial role in preventing the widespread transmission of pertussis. In our study, we used ROC and calibration plots to evaluate diagnostic effectiveness and validated its clinical net benefits through DCA. The model displayed fairly good discriminative ability for the training cohort, with an AUC of 0.741. The calibration curve showed fairly good agreement in training cohort and generally good in internal validation and external validation cohort.
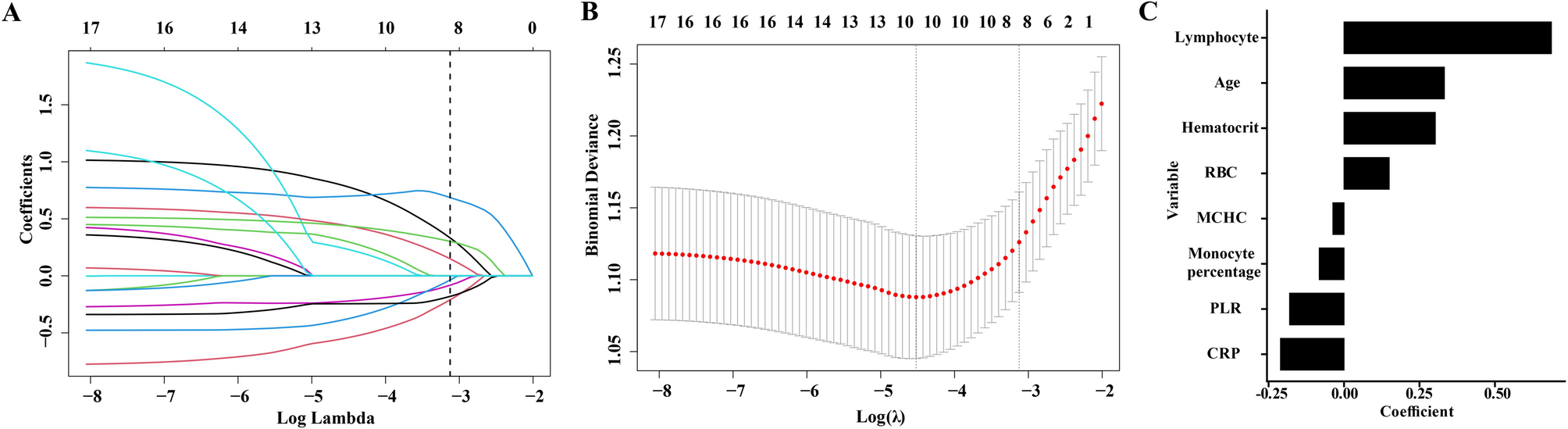
Our study identified higher age, lymphocyte count, hematocrit, and lower CRP as significant predictors of pertussis in children. We found that children older than 5 years are more susceptible to pertussis. The current immunization schedule in China is that infants should receive one dose of the combined vaccine against Tdap at 3 months, 4 months, 5 months, and 18 months of age [4]. The immunity provided by the vaccine may weaken over time, leaving older children vulnerable to pertussis. In addition, close contact between young children in confined spaces such as childcare facilities or schools also increases the risk of pertussis infection.
Blood cell markers had a good ability to predict pertussis. Previous studies have identified several biomarkers related to pertussis diagnosis, including white blood cells, lymphocytes, and neutrophils [20]. In this study, through the retrospective analysis of the laboratory characteristics of pertussis, we also found that lymphocyte was independent factors associated with pertussis. Pertussis toxin (PT) secreted by B. pertussis is a key factor in promoting lymphocyte proliferation [21]. PT activates a variety of cell signaling pathways through ADP ribosylation, promoting the release of lymphocytes from the bone marrow and spleen into the blood, resulting in an increase of peripheral blood lymphocytes [22]. In addition, pertussis infection triggers a strong immune response, especially the activation of CD4+ T lymphocytes.
Gao et al. found that hematocrit was independent factors associated with pertussis, which was consistent with our results [23]. In response to infections, the production of red blood cells within the bloodstream increases. This physiological adaptation could be an attempt to enhance oxygen delivery, which is essential for bolstering the immune system and facilitating tissue repair. Moreover, sever infections can trigger the release of inflammatory mediators that boost blood vessel permeability [24]. This allows fluid components to seep into the surrounding tissues, leading to a relative increase in the concentration of formed blood elements, which result in a relative rise in hematocrit levels consequently. In line with the results of previous studies [25], CRP was not significantly elevated in children with pertussis in our study. As a traditional bacterial marker, the underlying mechanism remains ambiguous and requires additional investigation.
Tozzi et al. developed an algorithm based on clinical symptoms, including a suspicion of pertussis by a physician, whooping, cyanosis and absence of fever which had high predictive value for laboratory-confirmed pertussis, but the sensitivity was only 46.30% [26]. Daluwatte et al. also developed a machine learning model for pertussis based on signs and symptoms predicted pertussis with an area under the precision-recall of 0.24 [27]. The diagnostic efficacy of these models was not particularly good and they were not applicable to asymptomatic patients with pertussis. The model based on laboratory data established by Gao, which includes WBC, CRP and PDW-MPV-R, had good performance with AUC of 0.773 for the training cohort and 0.804 for the validation cohort, which indicated satisfactory discriminative ability [23]. However, a lack of multi-center clinical validation limited the external utility of the model. Another single-center retrospective study proposed a machine learning model combining pertussis symptoms and routine blood test results [28]. The AUC was 0.69, which was comparable to that in our study (0.741 for the training cohort, 0.694 for the internal validation, and 0.675 for the external validation cohort). Unfortunately, the authors transformed the continuous variables included in the study (such as white blood cell/lymphocyte count and CRP) into binary variables based on the cutoff values of published literature, which might affect the diagnostic efficacy of the model. For all we know, this was the first multi-center diagnostic model for pertussis based on laboratory data, which could assist the diagnosis and treatment of pertussis especially in underdeveloped areas of China and low-income Asian developing countries.
Our model also has some limitations in clinical applications. First, it merely served as a reference and cannot confirm pertussis presence as definitively as PCR tests. Second, retrospective data collection may have introduced selection bias and confounding factors. The constraints imposed by the sample size and potential data bias may lead to model instability or suboptimal performance. Third, our study just enrolled Chinese patients and the generality of our findings to non-Asian populations cannot be determined. Fourth, our model only incorporates laboratory data which was varied across disease stages, this may affect the accuracy of the model. Further studies are required to address these limitations and improve our model’s external utility in the future.