With the emergence of 18F-flurpiridaz positron emission tomography (PET) for myocardial perfusion imaging (MPI), multiple societies of nuclear medicine and cardiology have unveiled clinical guidelines that offer recommendations for optimizing imaging protocols as well as insights on image interpretation.
Developed by the Society of Nuclear Medicine and Molecular Imaging (SNMMI), the European Association of Nuclear Medicine (EANM), the American College of Nuclear Medicine (ACNM) and the American Society of Nuclear Cardiology (ASNC), the new guidelines were published earlier today by the Journal of Nuclear Medicine and the Journal of Nuclear Cardiology.
Here are nine key takeaways from the new guidelines.
- While physicians have traditionally utilized single-photon emission computed tomography (SPECT) for MPI, PET imaging offers enhanced spatial resolution, improved accuracy and increased capacity for quantitative evaluation of myocardial blood flow (MBF), according to the guideline authors.
- Indications for 18F-flurpiridaz PET MPI include detection of flow-limiting obstructive coronary artery disease (CAD) and chest pain assessment for individuals with intermediate to high probability of CAD; asymptomatic people with a > 20 percent 10-year risk for atherosclerotic cardiovascular disease (ASCVD); and quantitation of hyperemic MBF and myocardial flow reserve.
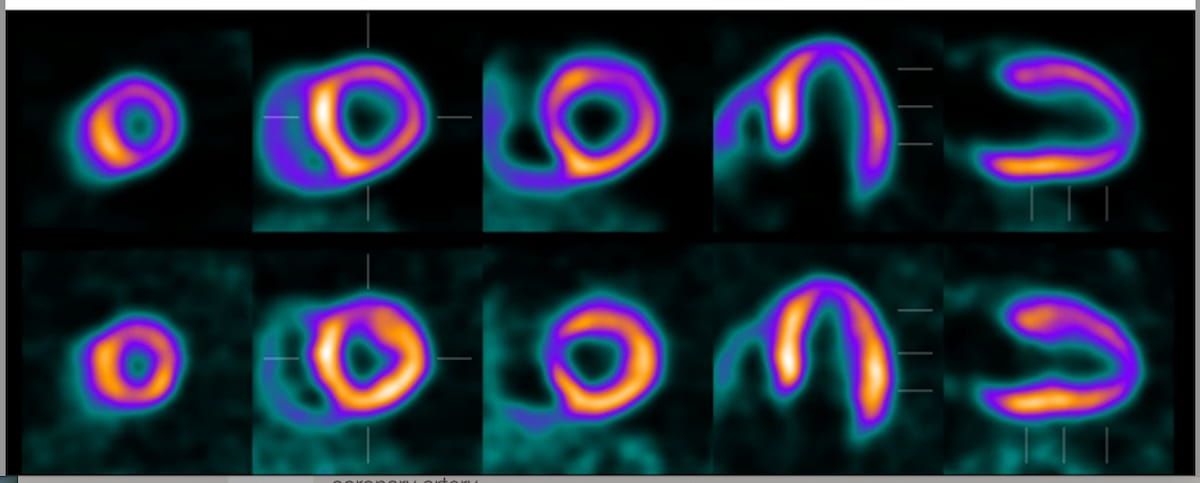
The high spatial resolution of 18F-flurpiridaz may magnify misregistration errors. In one case example, the appearance of an artifactual reversible perfusion defect in the anterior and lateral walls was caused by misregistration of 18F-flurpiridaz PET/CT at stress. (Images courtesy of SNMMI.)
3. In addition to access to 12-lead electrocardiograph and sphygmomanometer for stress test monitoring, the guideline authors noted that the PET/CT scanner should have cardiac electrocardiogram (ECG) gating.
4. Intravenous injection of 18F-flurpiridaz occurs at the patient’s peak exercise level, which the guideline authors define as > 85 percent age-adjusted maximal heart rate or maximal exertion. Employing a 10-minute list-mode acquisition protocol, the researchers emphasized obtaining PET imaging 15 to 25 minutes after the stress injection.
5. Conventional compartment modelling cannot be utilized after exercise stress to calculate stress MBF and myocardial flow reserve (MFR) given that distribution of the 18F-flurpiridaz PET agent has already occurred in the myocardium at the time of imaging, according to the guideline authors.
6. In order to prevent misalignment artifacts, the researchers suggest employing low-dose CT for attenuation correction of rest and stress imaging acquisitions.
7. By inspecting the fused display of PET and CT data, the guideline authors said one can prevent potential misregistration, which can lead to decreased MBF in the lateral, anterior and anterolateral regions.
8. Preliminary research has indicated that stress MBF may provide a slightly improved diagnostic assessment of lesions with 50 to 69 percent stenosis in comparison to relative perfusion alone, and possibly offers enhanced detection of epicardial CAD in contrast to MFR.
9. Through the quantification of resting and stress end-diastolic volume, ejection fraction and end-systolic volume, the researchers noted that 18F-flurpiridaz PET facilitates a thorough evaluation of left ventricular function.