Inclusion and exclusion criteria
Inclusion criteria: (i) Patients aged 65 years or older with FFPI type II or type IV pelvic fractures caused by low-energy trauma; (ii) Patients with a bone mineral density (BMD) T-score≤ -2.5 SD; (iii) Patients who have undergone RoRobot-assisted closed reduction and internal fixation, or TiRobot-assisted percutaneous cannulated screw fixation; (iv) Follow-up duration of at least 6 months; (v) Availability of complete clinical data.
Exclusion criteria: (i) Presence of open or old fractures (defined as fractures occurring more than 3 weeks ago, with delayed treatment or complications that result in delayed union, nonunion, or malunion); (ii) Presence of pathological fractures (e.g., bone metastases from cancer, primary bone tumors, or metabolic bone diseases); (iii) Inability to tolerate surgery; (iv) Mental illness that impairs the ability to cooperate with treatment and rehabilitation; (v) Severe pelvic fractures that cannot be reduced by closed methods; (vi) Patients with lower extremity trauma or fractures.
General information of patients
This retrospective study examined cases of unstable pelvic fractures in elderly patients with osteoporosis resulting from low-energy injuries, covering the period from October 2023 to May 2024. A total of 37 patients were included in the study. Based on the usability of the equipment, we adopted different surgical methods for eligible patients. Based on the usability of the equipment, we adopted different surgical methods for eligible patients.
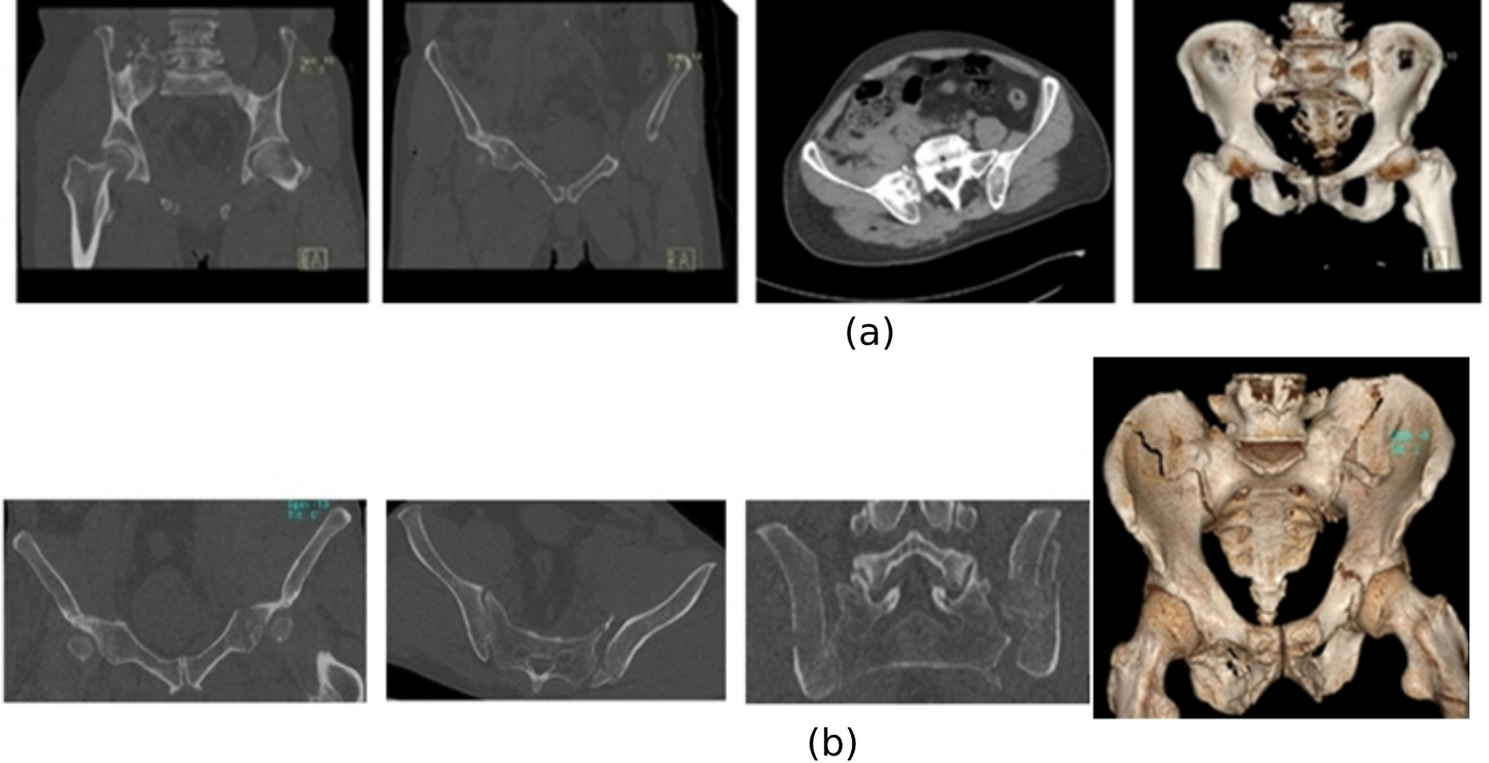
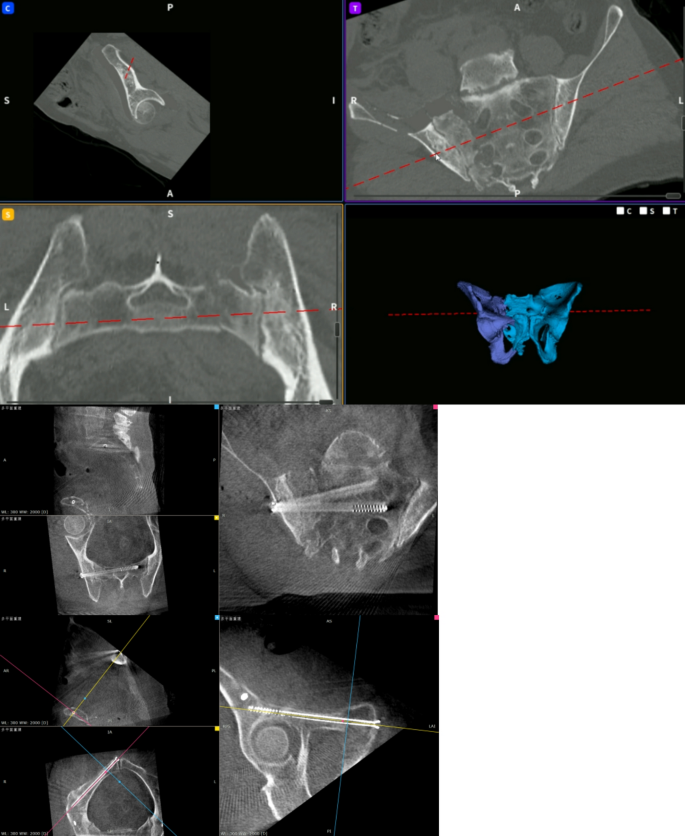
All patients underwent X-ray and CT scans prior to surgery to assess the treatment plan for pelvic fractures. Eighteen patients (8 males, 10 females; aged 65–81 years, with a mean age of 71.06 ± 4.22 years) received RoRobot-assisted closed reduction and internal fixation (RoRobot-assisted group). Nineteen patients who received TiRobot alone as adjunctive percutaneous cannulated screw fixation treatment during the same period were selected as the control group (TiRobot-assisted group). Among these, 7 males and 12 females, aged 66–78 years, with a mean age of 71.21 ± 3.54 years, were included. According to the FFP classification, type I refers to anterior injuries. Type II refers to non-displaced posterior injuries. Type III refers to displaced unilateral posterior injury, including IIIa, IIIb, and IIIc. Type IV refers to displaced bilateral posterior injuries, including IVa, IVb, and IVc. According to the FFP classification, the RoRobot-assisted group included 12 patients with type III and 6 patients with type IV injuries. The TiRobot-assisted group included 13 patients with type III and 6 patients with type IV injuries. (Fig. 1)
(a) CT image and ventral three-dimensional reconstruction of FFPIII pelvic fracture (b) CT image and ventral three-dimensional reconstruction of FFPIV pelvic fracture
Surgical procedure
Surgical procedure of RoRobot-assisted closed reduction and internal fixation
Eighteen patients in the RoRobot assistance group underwent fracture reduction surgery with the assistance of the Rossum Robot (Beijing Rossum Robot Technology Co., Ltd.). Three orthopedic surgeons specializing in pelvic trauma performed all surgeries, each having received professional training in operating intelligent robots. The steps are as follows:
General anesthesia was administered, followed by routine disinfection and preparation of sterile surgical instruments. For patients with type III and type IV pelvic fractures showing significant displacement, preoperative images were imported into the software, where the healthy and affected sides were marked and differentiated. The images of the healthy pelvic side were mirrored and registered. Using data processing and AI functions, precise automatic segmentation and reconstruction enabled personalized and quantitative planning for fracture reduction and screw placement.
The fusion and registration of preoperative and intraoperative image data enabled high-precision, real-time dynamic 3D visualization navigation during pelvic surgery. Real-time dynamic 3D visualization navigation allowed for precise and safe insertion of the holding needle using a handheld navigation drill, which displayed the position, angle, and depth of the needle insertion. The healthy and affected pelvic sides were securely fixed using the Rossum Tian Gong surgical robotic arm and the Rossum Wanxiang intelligent orthopedic robotic arm, while the Rossum Qingtian elastic electric orthopedic traction frame was attached to the patient’s lower limbs. The reduction position and path were previewed and the reduction plan confirmed. The Rossum Wanxiang intelligent orthopedic surgical robot’s unique force-position coordinated control mode enabled the safe closed reduction of pelvic fractures, guided by full-process, multi-angle, real-time visualization, monitoring, and automatic planning. An intelligent orthopedic surgical robot was then used to plan the screw channels and placements. Using a Rossum handheld guide, screw placement was completed precisely under real-time dynamic 3D visualization navigation, enabling minimally invasive treatment of pelvic fractures [18]. (Figures 2, 3, 4, 5 and 6)
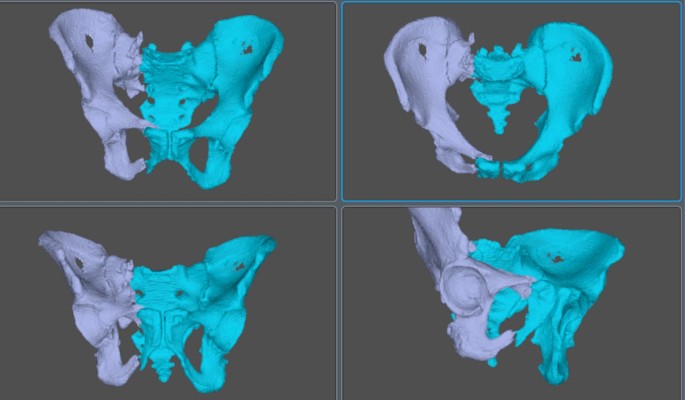
Fine-grained Automatic segmentation and reconstruction
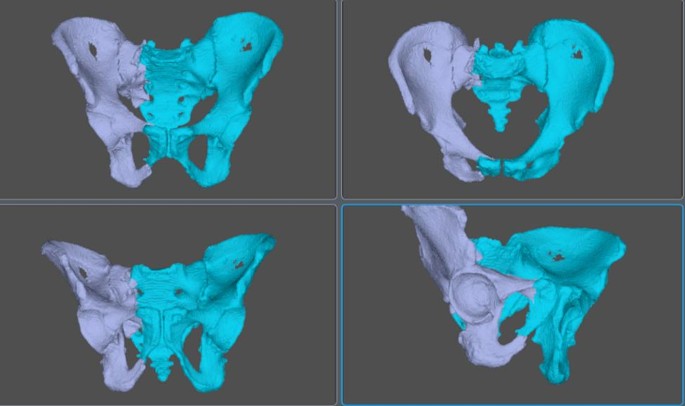
Artificial Intelligence Reset Planning
The force-position cooperative control mode achieves precise closed reset of the robot

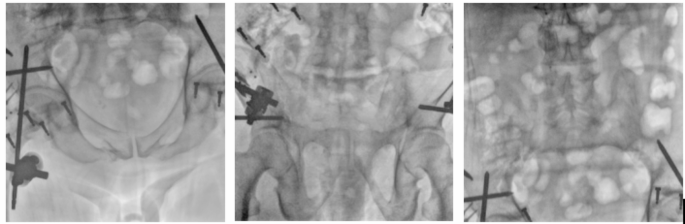
Real-time dynamic 3D visualization of needle placement
Real-time dynamic three-dimensional visualization navigation enables screw placement
TiRobot-assisted percutaneous cannulated screw fixation surgical procedure
Nineteen patients in the TiRobot-assisted surgery group were completed with the assistance of the second-generation orthopedic surgical robot (TiRobot ForcePro Superior, China) of Beijing Tianwei Medical Technology Co., Ltd.
All surgeries were performed by three orthopedic doctors specializing in pelvic trauma, and all of them received professional training in operating intelligent robots. The specific steps are as follows:
General anesthesia is administered. Routine disinfection and preparation of sterile surgical instruments are performed. For patients with significantly displaced type III and IV pelvic fractures, heavy traction of the lower extremities, external fixation screw implantation, and lever rotation are utilized. The TianJi orthopedic robot plans guide pin and screw channels of varying diameters for indirect reduction, thereby achieving minimally invasive closed pelvic reduction.
-
1)
3D Image Acquisition: The C-arm machine and optical tracking camera are used to acquire images, ensuring that the collected images include calibration points for scale and the bone structure to be treated. The 3D image of the pelvic area is then captured and transmitted to the main screen of the Dimensity orthopedic robot.
-
2)
Path Planning: Appropriate entry points and directions are selected to plan the placement of the target screws. The “Simulation” mode is activated, and the robotic arm is moved to the target position. A surgical incision of 0.5 to 1 cm is made along the position indicated by the robotic arm. Muscle tissue is then separated to expose the bone surface, and the guide pin sleeve is inserted until its tip contacts the bone surface.
-
3)
Hollow Screw Insertion: The Ti-Robot 2.0 system’s automatic execution mode is employed, enabling the robotic arm to sequentially place the guide pins and hollow screws along the sleeve direction according to the pre-planned length and direction. 3D images are then captured [7, 19, 20].
Observation indicators
Fracture reduction quality: The quality of pelvic fracture reduction post-surgery was assessed using the Matta scoring system [21]. The quality of pelvic fracture reduction post-surgery was assessed using the Matta scoring system [21]. Post-treatment, X-ray images of the anterior, inlet, and outlet views of the pelvis were obtained. The quality of pelvic fracture reduction was evaluated based on the maximum displacement measured by imaging. The Matta scoring system consists of four levels: A (excellent), defined as a fracture gap ≤ 4 mm; B (good), defined as a gap of 5–10 mm; C (fair), defined as a gap of 11–20 mm; and D (poor), defined as a gap > 20 mm. The excellent and good rate (EGR) of fracture reduction is calculated as (A + B) / (A + B + C + D) × 100%.
Screw placement accuracy rate (ASP): The accuracy of screw placement (ASP) was assessed using the Gras standard [22]. Screw implant positions are categorized into three grades: Grade I (good, safely placed, completely within the bone), Grade II (average, safely placed, in contact with cortical bone), and Grade III (poor, misaligned, penetrating cortical bone).ASP is calculated using the formula: (number of Grade I screws + number of Grade II screws) / total number of implanted screws × 100%.
Indicators for fracture healing include: ① No local tenderness or percussion pain. ② No abnormal local movement. ③ X-ray re-examination reveals a blurred fracture line with continuous callus bridging the fracture.
Postoperative pelvic function recovery: Postoperative pelvic function recovery was assessed using the Majeed score [23]. The Majeed score evaluates five aspects: working ability, pain level, sitting ability, standing ability, and sexual activity. The Majeed scoring system is based on a total of 100 points: 20 points for work ability, 30 points for pain level, 10 points for sitting ability, 36 points for standing ability, and 4 points for sexual activity. A total score of 85 or above indicates excellent recovery, 70 to 84 indicates good recovery, 55 to 69 indicates average recovery, and below 55 indicates poor recovery.
VAS score: The VAS is a widely used tool for assessing both subjective pain intensity and patients’ psychological perception [24]. A score of 0 represents no pain, while a score of 10 indicates intolerable extreme pain. In clinical assessment, scores ranging from 1 to 3 are categorized as mild pain, 4 to 6 as moderate pain, and 7 to 10 as severe pain. Lower scores correspond to milder symptoms.
Record the VAS and Majeed scores for patients before the operation, as well as 1 week, 1 month, 3 months, and 6 months postoperatively. Both patient groups followed the same postoperative rehabilitation and treatment regimen.
Postoperatively, all patients received analgesic and anticoagulant medications, as well as lower extremity venous pump training and other preventive measures.
Deep vein thrombosis (DVT) of the lower extremities was diagnosed. Postoperative treatment included calcium carbonate D3 for anti-osteoporosis, and preventive anti-infection therapy was administered within 24 h of surgery. A follow-up deep vein color Doppler ultrasound of the lower extremities was conducted within 24 h after surgery. Beginning 24 h post-surgery, the patient was assisted with mild hip flexion exercises 2–3 times daily, along with guidance on strengthening the lower extremities. Two weeks after surgery, the patient was instructed to actively bend the hip and knee joints while in bed. Four weeks post-surgery, the patient was guided to perform partial weight-bearing exercises with a walker. Twelve weeks post-surgery, when the fracture line had blurred significantly, the patient was instructed to perform full weight-bearing exercises.
Statistical analysis
The research data were analyzed using SPSS version 19 software. The data are presented as the mean ± SD or n (%) of the patients. The chi-square test, non-parametric test, and independent sample t-test were employed to compare demographic characteristics and clinical data across the groups. For correlation analysis, the Pearson correlation coefficient and Fisher’s exact test were used to assess the relationship between variables. All reported P-values were two-tailed, with a P-value < 0.05 considered statistically significant.