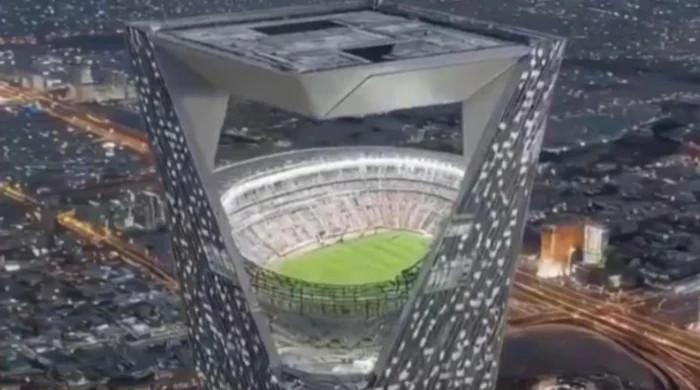
A viral AI-generated video showing a glowing ‘Sky Stadium’ high above the desert has misled millions of social media users into believing it was part of Saudi…
AI generated ‘Sky Stadium’ fake video tricks millions ahead of 2034 FIFA World Cup in Saudi Arabia – Football International