Global, regional, and national burden of cervical cancer in women of childbearing age (15–49 years) in 2021
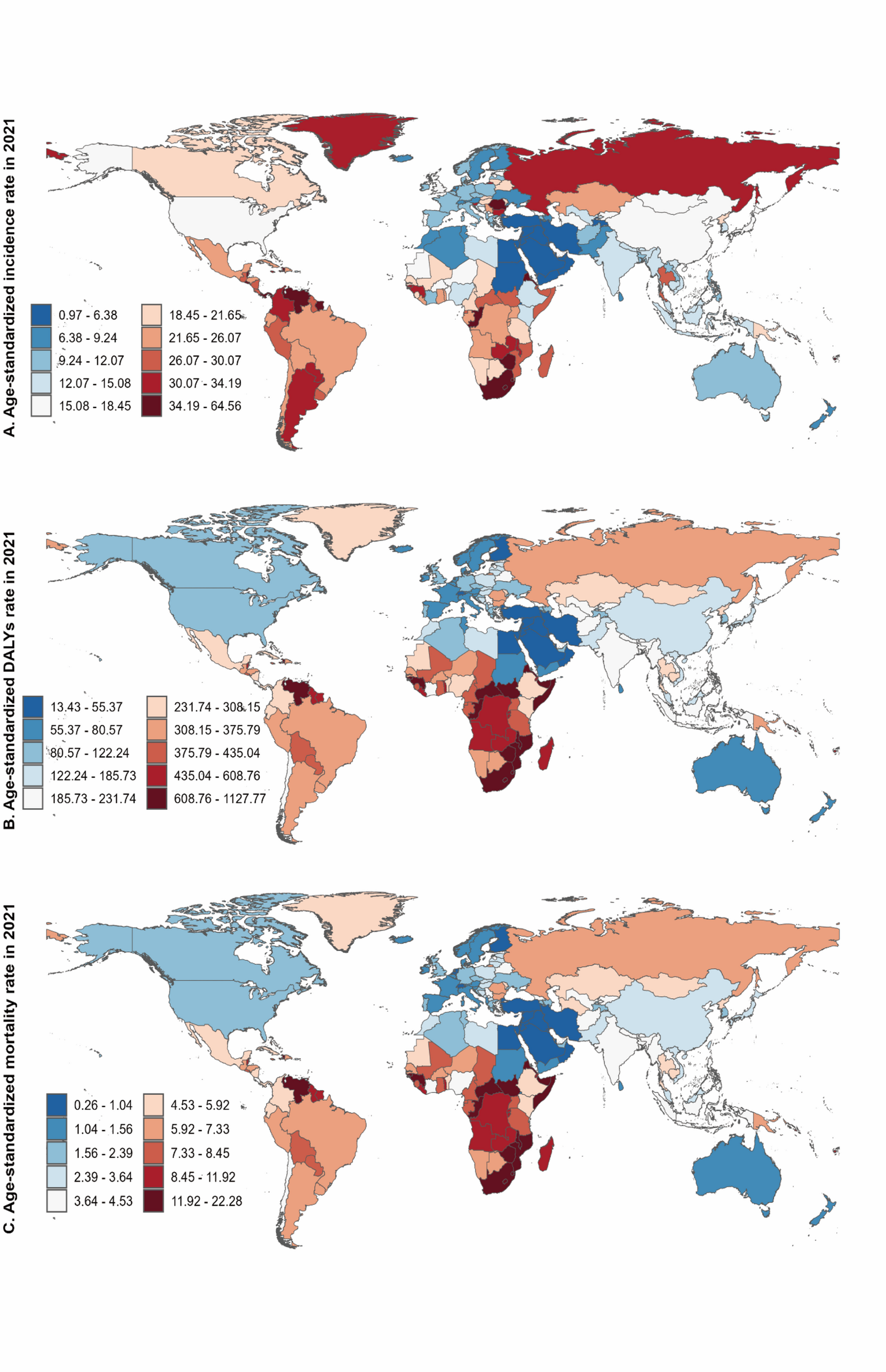
In 2021, notable geographical variations in the burden of cervical cancer were identified among women of childbearing age (15–49 years) across 204 countries and territories (Fig. 1). A comprehensive examination of 21 GBD regions revealed five regions with elevated ASIR: Southern Sub-Saharan Africa, Central Latin America, the Caribbean, Southern Latin America, and Andean Latin America (Fig. 1A). Southern Sub-Saharan Africa recorded the highest ASIR, exceeding 40 cases per 100,000, and also ranked among the regions with the highest ASDR, alongside Central Sub-Saharan Africa, the Caribbean, Eastern Sub-Saharan Africa, and Andean Latin America (Fig. 1B). The highest ASMR was observed in Southern Sub-Saharan Africa (Fig. 1C). Southern Sub-Saharan Africa exhibited an ASIR of 40.45 per 100,000 (95% UI: 33.74–47.03), an ASDR of 699.90 per 100,000 (95% UI: 584.46–813.42), and an ASMR of 13.83 per 100,000 (95% UI: 11.58–16.03).
At the country level, ASIR, ASDR, and ASMR varied considerably. The ASIR ranged from 0.97 per 100,000 (95% UI: 0.72–1.27) in Palestine to 64.56 per 100,000 (95% UI: 44.74–88.82) in Venezuela, while the ASDR ranged from 13.43 per 100,000 in Palestine (95% UI: 9.94–17.72) to 1,127.77 per 100,000 in Kiribati (95% UI: 760.97–1,632.40). Similarly, Palestine had a significantly lower ASMR of 0.26 per 100,000 (95% UI: 0.19–0.34), while Kiribati recorded a considerably higher ASMR of 22.28 per 100,000 (95% UI: 15.05–32.49).
Age-standardized rates of incidence (A), DALYs (B), and mortality (C) of cervical cancer in women of childbearing age (15–49 years) were analyzed across 204 countries and territories for the year 2021
Global and regional trends in cervical cancer ASPR in women of childbearing age (15–49 years), 1990–2021
From 1990 to 2021, the ASPR of cervical cancer in women of childbearing age (15–49 years) increased gradually, from 91.60 per 100,000 (95% UI: 86.20–97.40) to 105.00 per 100,000 (95% UI: 96.40–114.00). These data indicate a notable upward trend in the prevalence of cervical cancer (Table 1; Fig. 2A). However, this overall increase masks significant variations across age groups, highlighted by the average annual percentage change (AAPC) values. For example, in the youngest group (15–19 years), ASPR rose modestly from 5.85 per 100,000 (95% UI: 5.16–6.53) to 6.28 per 100,000 (95% UI: 5.42–7.57) over the period, with an AAPC of 0.23 (95% CI: -0.01 to 0.46; P = 0.055). The 20–24 age group saw a more noticeable increase, with ASPR increasing from 16.50 per 100,000 (95% UI: 15.00–18.50) to 18.70 per 100,000 (95% UI: 16.50–21.50) and an AAPC of 0.40 (95% CI: 0.35–0.44; P < 0.001). Although cervical cancer in women under 25 years is rare, it often presents with aggressive subtypes—such as adenosquamous or small-cell carcinoma—and carries a poorer prognosis. Conversely, the ASPR for women aged 25–29 remained stable, with an AAPC of 0.01 (95% CI: -0.29 to 0.31; P = 0.953). However, declines were observed in the 30–34 and 35–39 age groups, with ASPR decreasing from 127.00 to 120.00 and from 177.00 to 171.00 per 100,000, respectively, featuring AAPCs of -0.18 (95% CI: -0.21 to -0.15; P < 0.001) and − 0.09 (95% CI: -0.12 to -0.07; P < 0.001). In contrast, the 40–44 age group experienced a slight increase in ASPR from 201.00 per 100,000 (95% UI: 188.00–215.00) to 205.00 per 100,000 (95% UI: 188.00–223.00) (AAPC: 0.06, 95% CI: 0.02–0.09; P = 0.006), and the 45–49 age group also saw a rise from 189.00 per 100,000 (95% UI: 177.00–202.00) to 198.00 per 100,000 (95% UI: 179.00–221.00) (AAPC: 0.15, 95% CI: 0.12–0.17; P < 0.001).
The global burden of cervical cancer rose significantly, with cases increasing by 67% from 1.23 million (95% UI: 1.15–1.30) in 1990 to 2.05 million (95% UI: 1.88–2.23) in 2021 (Table 1). Despite the rise in absolute numbers, the global AAPC was modest at 0.45% (95% CI: 0.43–0.47, P < 0.001), indicating a gradual increase in ASPR up to 2021 (Table 1; Fig. 2A). Nevertheless, this global pattern masks significant regional variations among SDI quintiles.
The examination of SDI regions revealed distinct trends, as high-middle, middle, and low-middle SDI regions showed increases over three decades (AAPC > 0) (Table 1). The high-middle SDI region demonstrated significant growth, with the ASPR increasing from 74.70 per 100,000 (95% UI: 68.80–80.80) in 1990 to 124.00 per 100,000 (95% UI: 106.00–142.00) in 2021. This yielded the highest AAPC of 1.67 (95% CI: 1.62–1.73; P < 0.001) (Table 1; Fig. 2C). The middle SDI region exhibited a notable increase from 76.60 per 100,000 (95% UI: 70.00–83.60) to 112.00 per 100,000 (95% UI: 100.00–125.00) (AAPC: 1.27, 95% CI: 1.07–1.46; P < 0.001) (Table 1; Fig. 2D). In contrast, the low-middle SDI region experienced a moderate rise from 82.30 per 100,000 (95% UI: 72.10–93.60) to 91.00 per 100,000 (95% UI: 80.10–102.00) (AAPC: 0.32, 95% CI: 0.27–0.37; P < 0.001) (Table 1; Fig. 2E). Both the high SDI and the low SDI regions exhibited declining trends. The high SDI region experienced a reduction in ASPR from 147.00 per 100,000 (95% UI: 144.00–151.00) to 105.00 per 100,000 (95% UI: 102.00–108.00) (AAPC: -1.10, 95% CI: -1.13 to -1.07; P < 0.001) (Table 1; Fig. 2B). Meanwhile, the low SDI region recorded a decrease from 103.00 per 100,000 (95% UI: 86.40–124.00) to 94.60 per 100,000 (95% UI: 78.40–114.00) (AAPC: -0.32, 95% CI: -0.35 to -0.29; P < 0.001) (Table 1; Fig. 2F). These heterogeneous patterns underscore regional differences in the prevalence of cervical cancer across different SDI regions.
Age-specific analysis of cervical cancer ASPR across SDI regions in women of childbearing age (15–49 years), 1990–2021
From 1990 to 2021, our analysis identified varied age-specific patterns in cervical cancer prevalence across different SDI regions (Fig. 2A–F). Throughout these regions, age-related trends followed a consistent pattern, with the 15–19 age group exhibiting the lowest ASPR, while the 40–44 age group recorded the highest ASPR. Globally, the ASPR for the 40–44 age group reached a peak in 2018 at 208.13 per 100,000 (95% UI: 192.99–224.00) (Fig. 2A). The greatest changes were observed in the high SDI region during this period. Notably, in this region, the ASPR for the 40–44 age group decreased from 239.48 per 100,000 (95% UI: 230.54–249.00) in 1990 to 170.33 per 100,000 (95% UI: 161.62–179.47) in 2021 (Fig. 2B). Meanwhile, the high-middle SDI region experienced less pronounced fluctuations, with a decline noted as the ASPR in the same age group dropped from 226.38 per 100,000 (95% UI: 198.40–256.97) in 2018 to 218.02 per 100,000 (95% UI: 188.26–253.85) by 2021 (Fig. 2C). In the middle SDI region, the 40–44 and 45–49 age groups reached their highest rates in 2021, at 216.46 per 100,000 (95% UI: 192.80–243.72) and at 214.50 per 100,000 (95% UI: 189.06–245.34), respectively (Fig. 2D). Conversely, in the low-middle SDI region, the ASPR for the 40–44 age group decreased from 204.37 per 100,000 (95% UI: 173.92–236.81) to 195.79 per 100,000 (95% UI: 171.08–222.15) (Fig. 2E). More dramatically, the low SDI region reported a substantial reduction in ASPR from 249.49 per 100,000 (95% UI: 203.50–305.03) in 1990 to 213.74 per 100,000 (95% UI: 174.26–266.01) in 2021 (Fig. 2F).
Overall, the ASPR showed a similar pattern globally and across SDI regions, with older groups (35–39 years, 40–44 years, 45–49 years) showing higher ASPR than younger groups (15–19 years, 20–24 years, 25–29 years, 30–34 years).
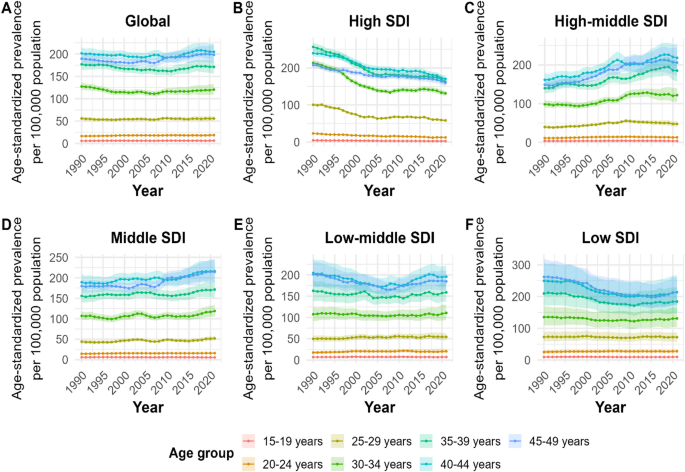
Trends in ASPR of cervical cancer from 1990 to 2021 globally and across regional levels, segmented by age groups among women of childbearing age (15–49 years): 15–19, 20–24, 25–29, 30–34, 35–39, 40–44, and 45–49 years. Panels: A (Global), B (High SDI), C (High-middle SDI), D (Middle SDI), E (Low-middle SDI), and F (Low SDI)
Joinpoint regression analysis of global and regional ASPR trends in women of childbearing age (15–49 years), 1990–2021
We applied Joinpoint regression to evaluate trends in the age-standardized prevalence rate (ASPR) of cervical cancer among women aged 15–49 years. Analyses covered the period 1990–2021 at the global level and across SDI regions (Fig. 3A–F). Globally, the analysis revealed four distinct joinpoints occurring in 1995, 2007, 2014, and 2017 (Fig. 3A). Initially, from 1990 to 1995, the ASPR increased, with an APC of 0.35% (95% CI: 0.22–0.62%; P = 0.005). However, from 1995 to 2007, the increase was not statistically significant, with a change of 0.08% (95% CI: -0.05–0.13%; P = 0.087). Subsequently, a slight upward trend of 0.87% was noted from 2007 to 2014 (95% CI: 0.15–0.95%; P = 0.021), followed by a more marked increase from 2014 to 2017 (APC = 1.28%, 95% CI: 0.97–1.43%; P < 0.001). After 2017, the growth moderated, with an APC of 0.29% from 2017 to 2021 (95% CI: 0.03–0.45%; P = 0.034).
In the high SDI region, the ASPR showed a downward trend, with key joinpoints occurring in 1996, 2002, 2005, 2016, and 2019 (Fig. 3B). The decline from 1990 to 1996 was notable at an APC of -0.75% (95% CI: -0.99% to -0.56%; P = 0.004), which intensified to -2.61% from 1996 to 2002 (95% CI: -2.89% to -0.68%; P < 0.001). From 2002 to 2005, the trend continued to decline at -1.89% (95% CI: -2.73% to -0.36%; P = 0.009), and from 2005 to 2016, a minor negative trend remained at -0.09% (95% CI: -1.91–0.19%; P = 0.180). A significant decline was then observed from 2016 to 2019, with an APC of -0.85% (95% CI: -1.05% to -0.06%; P = 0.026), and the most pronounced negative change occurred from 2019 to 2021, at an APC of -2.24% (95% CI: -2.78% to -1.52%; P < 0.001).
In contrast, the high-middle SDI region demonstrated a steady upward trajectory, with significant changes identified at joinpoints in 1994, 2002, 2005, and 2018 (Fig. 3C). From 1990 to 1994, the APC in ASPR of cervical cancer climbed sharply by 2.37% (95% CI: 1.92–3.22%; P < 0.001). This increase continued from 1994 to 2002, where APC reached 1.49% (95% CI: 0.93–1.65%; P < 0.001). Subsequently, APC increased to 3.38% from 2002 to 2005 (95% CI: 2.57–3.73%; P < 0.001). From 2005 to 2018, however, the growth rate moderated at an APC of 1.71% (95% CI: 1.60–1.80%; P < 0.001). A slight decline was observed from 2018 to 2021, with a non-significant decrease in APC of -0.59% (95% CI: -1.46–0.12%; P = 0.106). Similarly, the middle SDI region increased, with joinpoints in 2004 and 2007 (Fig. 3D). Initially, from 1990 to 2004, APC surged significantly by 1.48% (95% CI: 1.38–1.57%; P < 0.001). The trend then displayed a non-significant decline from 2004 to 2007, with a change of -0.67% (95% CI: -2.65–1.35%; P = 0.497). Subsequently, from 2007 to 2021, APC increased again to 1.48% (95% CI: 1.38–1.57%; P < 0.001).
The low-middle and low SDI regions exhibited a decline followed by increases. In the low-middle SDI region, a single joinpoint was detected in 2007 (Fig. 3E). From 1990 to 2007, there was a significant decline of 0.24% (95% CI: -0.36% to -0.14%; P < 0.001), but from 2007 to 2021, the trend reversed, with an APC increase of 1.01% (95% CI: 0.88–1.17%; P < 0.001). In the low SDI region, joinpoints occurred in 1999, 2003, and 2010 (Fig. 3F). From 1990 to 1999, there was a notable decline of 0.59% (95% CI: -0.71% to -0.45%; P < 0.001), deepening to -1.98% from 1999 to 2003 (95% CI: -2.50% to -1.56%; P < 0.001) and continued at -0.40% from 2003 to 2010 (95% CI: -0.65% to -0.14%; P = 0.008). From 2010 to 2021, a significant increase of 0.56% was observed (95% CI: 0.47–0.68%; P < 0.001).
These diverse temporal patterns across different SDI regions indicated complex underlying dynamics, prompting further investigation into age, period, and cohort effects.
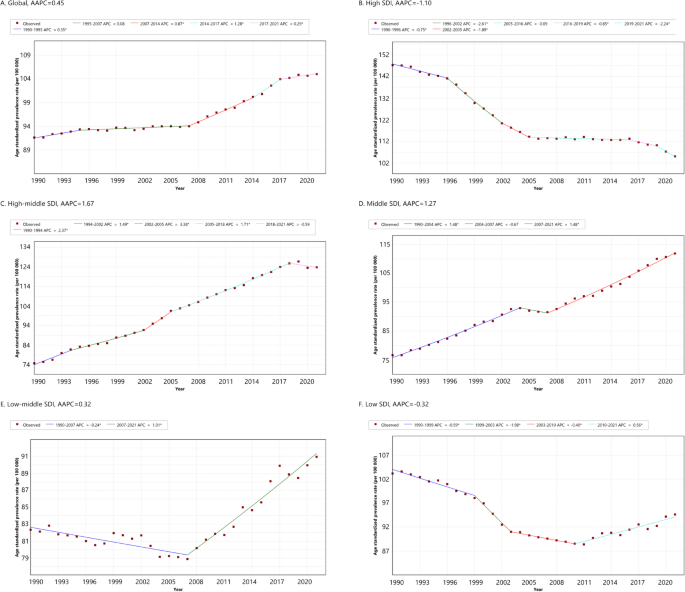
Joinpoint regression analysis of cervical cancer ASPR in women of childbearing age (15–49 years) at global and regional levels, 1990–2021. Panels: A (Global), B (High SDI), C (High-middle SDI), D (Middle SDI), E (Low-middle SDI), F (Low SDI). AAPC, average annual percentage change; APC, annual percentage change
Projected age-standardized prevalence rate of cervical cancer, 2021–2030
Using the most recent APC segments, we projected the age-standardized prevalence rate (ASPR) of cervical cancer in women aged 15–49 years. Projections cover 2021–2030 across all SDI regions (Fig. 4). The projections reveal distinct regional trends: projected ASPR values are expected to increase in middle SDI, low-middle SDI, and low SDI regions, particularly in the middle SDI group (APC = 1.48%). In contrast, a declining trend is projected in the high SDI and high-middle SDI regions, particularly in the high SDI region (APC = -2.24%). Globally, ASPR is projected to increase modestly, from 105.00 per 100,000 in 2021 to approximately 108.30 per 100,000 by 2030. The shaded areas in the figure represent the 95% confidence intervals (CIs) around the projections. These intervals reflect the uncertainty inherent in trend extrapolation and indicate that future cervical cancer burden is likely to vary substantially by region.
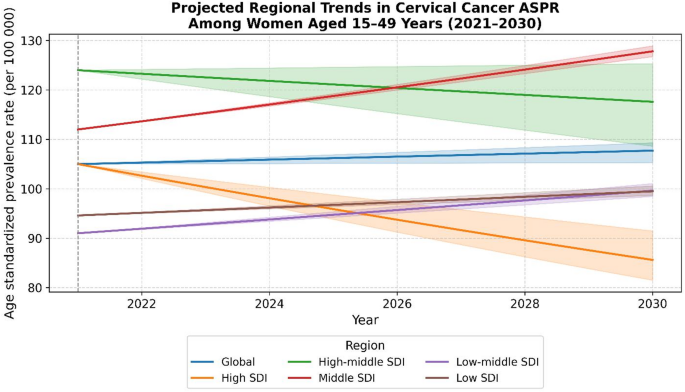
The projected ASPR of cervical cancer across SDI regions from 2021 to 2030 based on Joinpoint-derived APCs
Global and regional age, period, and cohort effects on cervical cancer ASPR in women of childbearing age (15–49 years), 1990–2021
Within the age-period-cohort framework, cervical cancer risk increases with age, peaks, and then declines slightly, yet remains highest in older age groups. The age effect on the ASPR of cervical cancer for women aged 15–49 was shown to follow a consistent pattern across all SDI regions (Fig. 5A). The ASPR exhibited a gradual increase with advancing age, reached its peak in the 40–44-year age group across the global population and in the majority of SDI regions, and was followed by a slight decline. In the region with high SDI, the age of peak ASPR occurred earlier, specifically at 35–39 years, after which there was a significant decline. The observed patterns indicate a clear trend of rising prevalence as age increased, coupled with significant variations across different regions. Contrary to the expectation that the lowest SDI quintile would uniformly have the highest ASPR across all age groups, regions with low SDI showed the highest ASPR for cervical cancer in most age groups, reflecting a significant burden.
Globally, cervical cancer ASPR remained constant over the earliest and most recent periods, with RR1990–1991 = 1.07 (95% CI: 1.04–1.11) and RR2017–2021 = 1.07 (95% CI: 1.04–1.09), both featuring overlapping 95% confidence intervals. Nevertheless, distinct regional trends became apparent. The high SDI region exhibited the most pronounced decrease, with the RR falling from 1.47 (95% CI: 1.44–1.50) to 0.94 (95% CI: 0.92–0.95). In contrast, the high-middle SDI region exhibited a consistent increase from 0.90 (95% CI: 0.88–0.93) to 1.13 (95% CI: 1.11–1.16), while the middle, low-middle, and low SDI regions displayed moderate fluctuations (Fig. 5B).
The global birth cohort effect showed a relatively stable ASPR across various cohorts, with significant differences across SDI regions (Fig. 5C). Earlier cohorts in the high, low-middle, and low SDI regions exhibited elevated ASPR. Interestingly, the 2000–2005 birth cohort in the high SDI region exhibited a significantly reduced relative risk (RR = 0.51, 95% CI: 0.41–0.64) compared to the corresponding cohorts in other SDI regions. These findings revealed significant regional and temporal variations in cervical cancer prevalence.
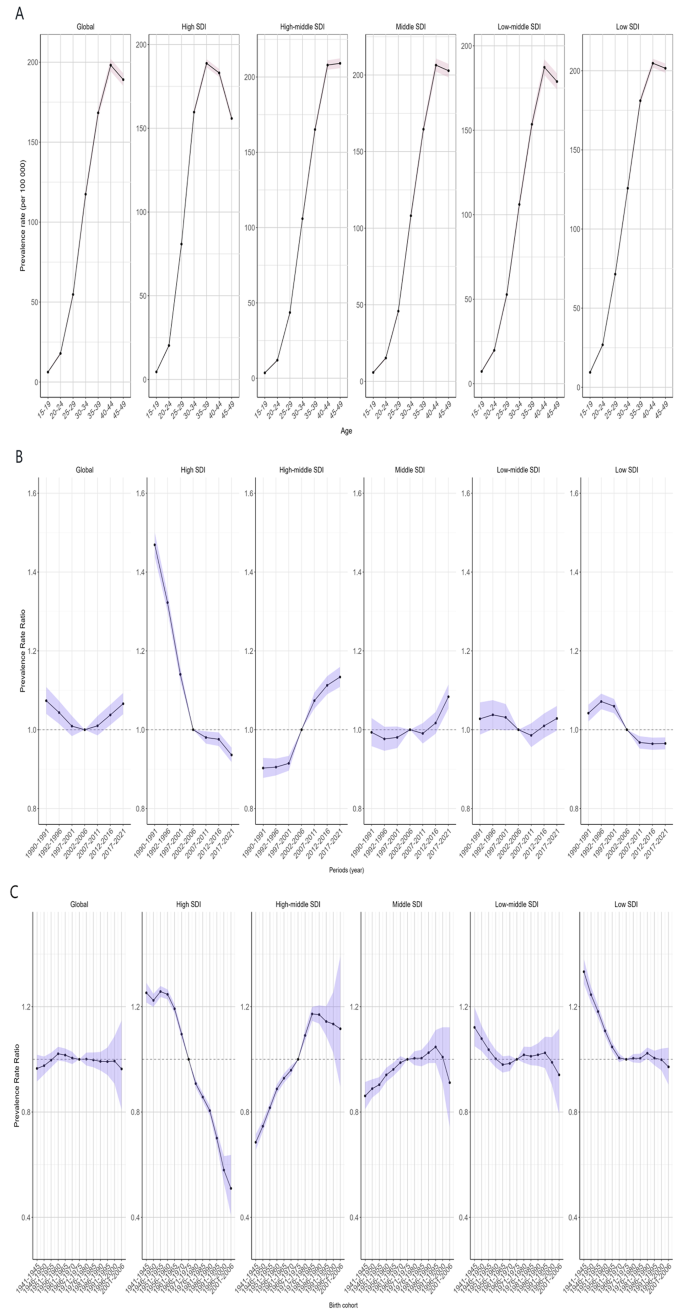
The age-period-cohort analysis of cervical cancer ASPR in women of childbearing age (15–49 years) in global and SDI regions. Panels: A (longitudinal age curve of prevalence), B (period rate ratio of prevalence), C (cohort rate ratio of prevalence)