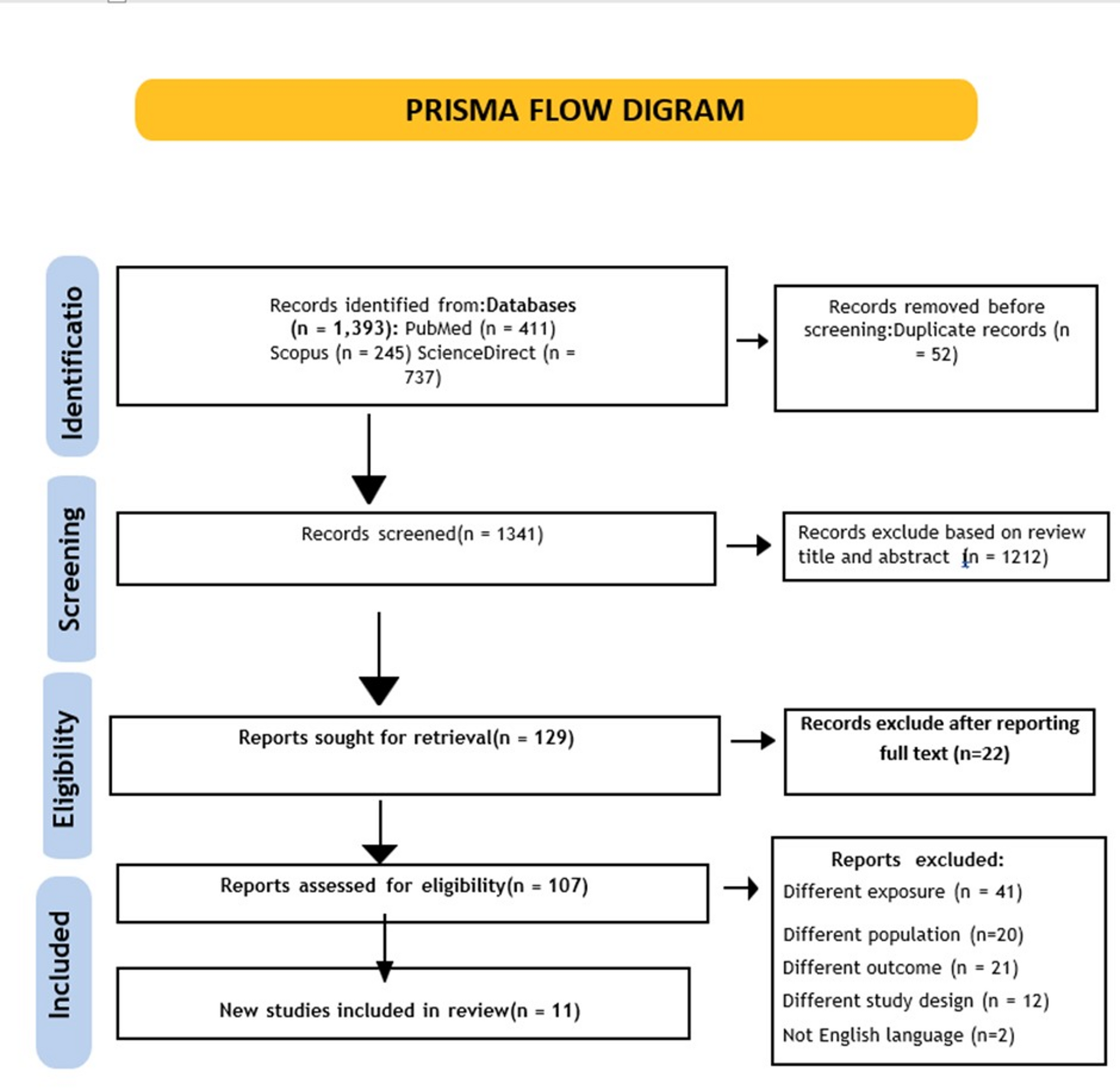
The electronic search identified a total of 1393 studies as shown in Fig. 1. After removing the duplications, the titles and abstracts of 1341 studies underwent eligibility assessment, followed by the full-text analysis of 107 studies. Of these, 96 were considered inappropriate for inclusion because they evaluated various populations (n = 20) or exposures (n = 41), had different outcomes in the studies as shown by n = 21 had different study designs as represented by n = 12, or the studies were not conducted in English, n = 2. Eleven individual studies formed the basis of this review.
PRISMA Flow Diagram of Selection Studies
Table 1 provides an overview of the participants’ characteristics for the eleven included studies in chronological order and by study design. Eight studies were cross-sectional [10, 23,24,25,26,27,28,29]. One was a quantitative cross-sectional survey with a mixed-methods design [30], and two were prospective cohorts [31, 32].
This analysis included data from various LMICs across several regions. One study focused on data from specific countries in Southeast Asia, such as Myanmar [27]. Data from multiple Asian countries, including India [28, 32], Bangladesh [30], Nepal [23], and China [29] were analysed in a separate study. The remaining studies investigated data from individual countries in various regions: Romania [31] in Eastern Europe, Brazil [25, 26] in Latin America, South Africa in Sub-Saharan Africa [24], and a study from Ethiopia in East Africa [10].
The number of participants varied from 46 [31] to 1252 TB patients [29]. Across all studies, men comprised the majority of participants [10, 23, 25,26,27,28,29,30,31,32]. However, the South African study included only male participants [24]. The mean age varied from 32.69 to 46 years old.
Risk of bias
There was a moderate risk of bias in eight studies [23,24,25,26, 28, 31,32,33], and a low risk of bias in three studies [10, 27, 29]. In the majority of included studies, the confounding factors were not identified. Such oversight resulted in a significant amount of moderate bias in the majority of the results as shown in Tables 2 and 3.
Depression measurement tools
All included/eligible studies measured depression symptoms using a quantitative self-reported psychometric instrument that was validated for the tuberculosis patients.
Six studies employed the 9-item Patient Health Questionnaire (PHQ-9) measure for depression, which was the most often utilised questionnaire [10, 23, 25,26,27,28, 32]. Furthermore, one study [31] employed the 14-item Hospital Anxiety and Depression Scale (HADS), which consists of seven items for each depression subscale. Another study combined the use of the 14-item HADS with the 9-item Patient Health Questionnaire (PHQ-9) [29]. One study made use of the Structured Clinical Interview for the DSM-IV (SCID) [30]. For the assessment of depression, a scale that included measurements from the Kessler Psychological Distress Scale [24] and the Study Short Form-36 (SF-36) version 2 was employed [25].
Smoking and depression
Cross-sectional studies
Most studies conducted across different geographical regions found a strong association between smoking and depression.
Table 4 demonstrates that from 9 cross-sectional studies, 5 studies found an increased risk of depression associated with smoking among tuberculosis patients in many countries, such as Ethiopia, Nepal, South Africa, Brazil, and India all showed that smokers have significantly higher rates of depression as compared to non-smokers [10, 23,24,25, 28].
According to Ethiopian research, smokers had 9.08 times higher rates of depression than non-smokers [AOR = 9.08; 95% CI (3.35, 24.61); p < 0.001] [10]. In a similar vein, research conducted in Nepal found that PHQ-9 scores were much higher among current smokers than in nonsmokers. [P = 0.02; B = 1.379] [23]. Furthermore, Indian research found that the prevalence of depression among TB tobacco users is 67.7%, with a p-value = 0.00001 in non-smokers [28]. Furthermore, research with a large sample size of 1005 patients carried out in South Africa found a statistically significant correlation (p-value = 0.017) between current tobacco use and depression, with around one-third (33.5%) of the patients receiving a diagnosis [24].
Similarly, Brazilian research found that there was a significant difference (p = 0.008) in HADS scores between current and former smokers and non-smokers. Proportion of depression among patients who did not have depression (15.3%) were significantly lower compared to the proportion of TB patients who were current smokers and had depression (44%) [25].
A study conducted in Myanmar found that the PHQ-9 ratings of smokers with depression were not substantially different from those of non-smokers. Former smokers (n = 9 (7.38%), AOR = 0.59; 95% CI (0.27, 1.32)), current smokers were (n = 1 (25%) [AOR = 2.49; 95% CI (0.25, 24.87) p = 0.29), non-smokers (n = 24 (11.82%) AOR = 1), former smokers were less likely to have depression than never smokers; however, current smokers might be more likely to have depression than non-smokers [27]. The associations of non-smokers, former smokers, and current smokers with depression did not differ according to additional studies conducted in China, Bangladesh, and Brazil [26, 29, 30].
Out of eleven studies, only two of them compared depression risk between current and former smokers, despite trends indicating more likelihood of depression among current smokers [27, 29].
Cohort studies
Although five cross-sectional studies revealed that there is an association between smoking and depression among TB patients, two cohort studies found that there was no association between current smoking status and depression [31, 32]. These differences in findings may be caused by the small sample sizes of the cohort studies (46 and 86 patients), compared to the numbers in the cross-sectional studies. Smaller samples lack adequate power to observe differences. Researchers reported that smokers experienced higher rates of stress and depression, but the p-value of 0.19 did not indicate statistical significance [32]. To evaluate depressive symptoms, the nine-item Patient Health Questionnaire (PHQ-9) depression scale was used. Three visits were made to screen for depression via the PHQ-9 questionnaire. When the groups that received counselling or medication and had psychiatric referrals between the initial visit and final visit were compared, there was a statistically significant difference in the mean PHQ-9 score (p = 0.001). Following a psychiatric evaluation, patients who were started on medication had a decrease in the PHQ-9 score that was not statistically significant (8.85 ± 5.45 and 8.83 ± 5.07, p = 0.053) [32].
Meta-analysis
Initially, only 4 studies reported adjusted odds ratio calculation in multivariate analysis for the association of smoking and depression out of 11 reviewed articles [10, 23, 29, 30],. On the other hand, univariate analysis was performed in 3 articles, and in 4 articles, only p-values were reported without the calculation of effect sizes. To maximize the inclusion studies, we contacted the corresponding authors of the remaining studies for unreported data, but only one provided partial data related to multivariate analysis that we included in our analysis [26].
Due to the lack of multivariate-adjusted effect size and inability to obtain unreported data, only five studies were included in the meta-analysis, all of them were cross-sectional studies as shown in Fig. 2 which demonstrates the random effects model result about the association between smoking and depression among tuberculosis (TB) patients and reveals that smoking TB patients have approximately 2.56 times more depression than non-smoking TB patients. The smoking habit in TB patients was significantly associated with depression; p = 0.003.
A forest plot was generated using RevMan 5.3. The result of the heterogeneity statistic (I2 = 71%) shows a high degree of heterogeneity across the included studies in the meta-analysis, which means that there is variation in the effect sizes between the different studies. This difference likely arises from a mix of factors, including the various tools used to measure depression (like PHQ-9, DSM, and HADS), the sizes of the samples, the types of tuberculosis, the cultural backgrounds, and some confounding factors that we just couldn’t measure.
Publication bias
Publication bias was assessed by the Eggers test using Stata MP 64-bit, version 13.0 (StataCorp LLC, College Station, TX, USA). There was no indication of publication bias, as Egger’s test suggested (bias coefficient = 0.59, p = 0.874). However, since only five studies were included in the analysis, the power of the test may have been compromised to detect asymmetry; therefore, this result should be treated with caution.
Subgroup analysis
Subgroup analysis was conducted based on depression measurement tools applied in the studies. Four studies utilized the PHQ-9 tool [10, 23, 26, 29], and one study utilized DSM-IV (SCID) [30]. The PHQ-9 subgroup also had a statistically significant correlation between smoking and depression (OR = 3.36; 95% CI: 1.19–9.50; p = 0.002), but heterogeneity was high (I² = 75%). The DSM-IV tool study lacked a significant association (OR = 1.00; 95% CI: 0.37–2.70). Other preplanned subgroup analyses that were considered for this MA (e.g., TB type, region) could not be performed owing to the insufficient number of studies in the MA. High heterogeneity should be considered a significant drawback for the pooled estimates.
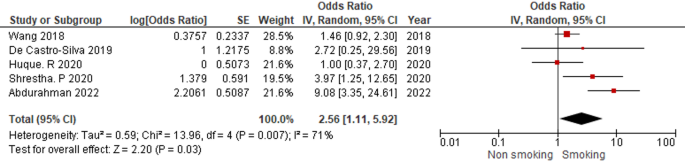
Forest Plot of the Association between Smoking and Depression among TB patients