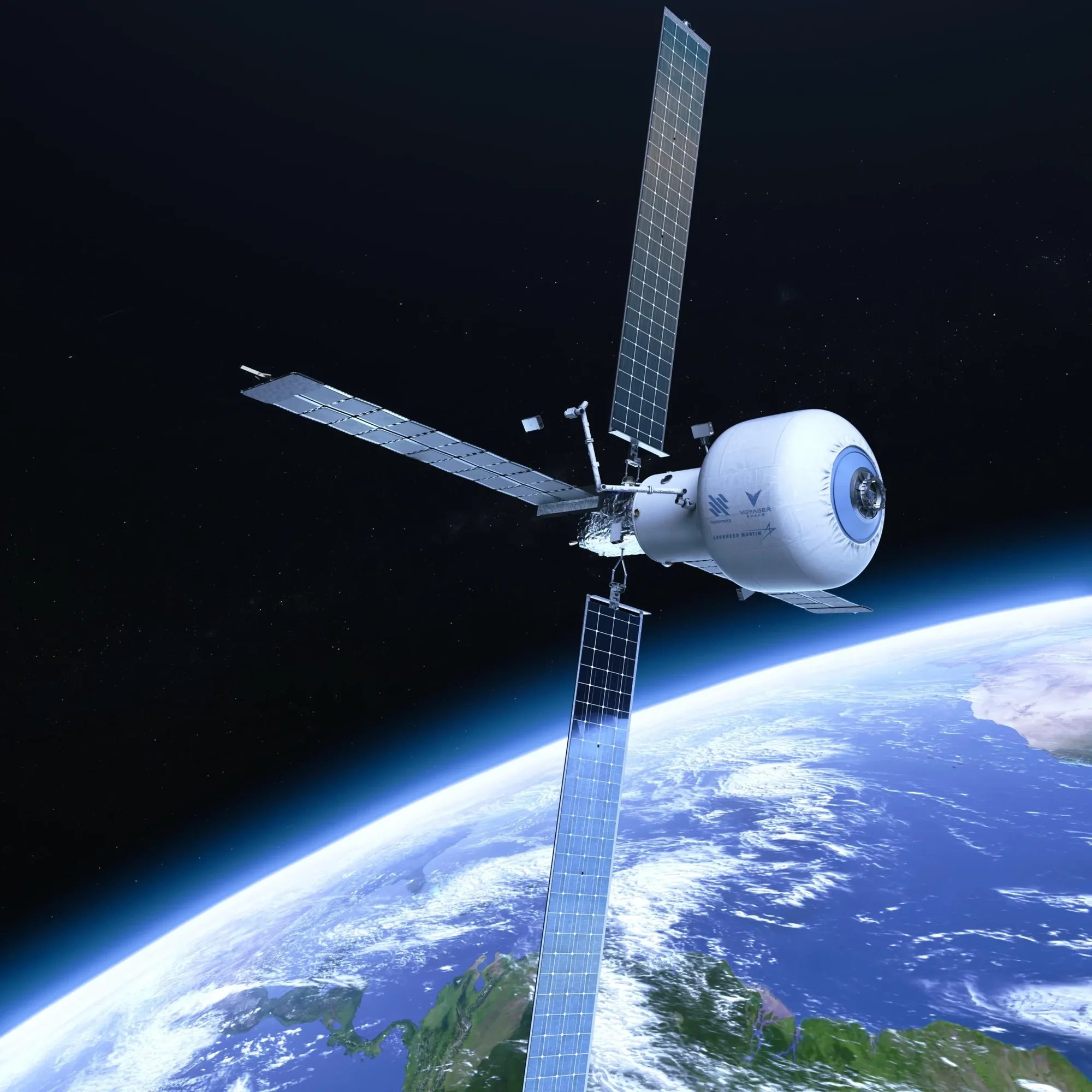
Commercial space stations are rapidly moving from concept to reality. As NASA prepares for the International Space Station’s retirement around 2030, a burgeoning private orbital industry could step into its shoes.
The ISS was humanity’s only…
Commercial space stations are rapidly moving from concept to reality. As NASA prepares for the International Space Station’s retirement around 2030, a burgeoning private orbital industry could step into its shoes.
The ISS was humanity’s only…
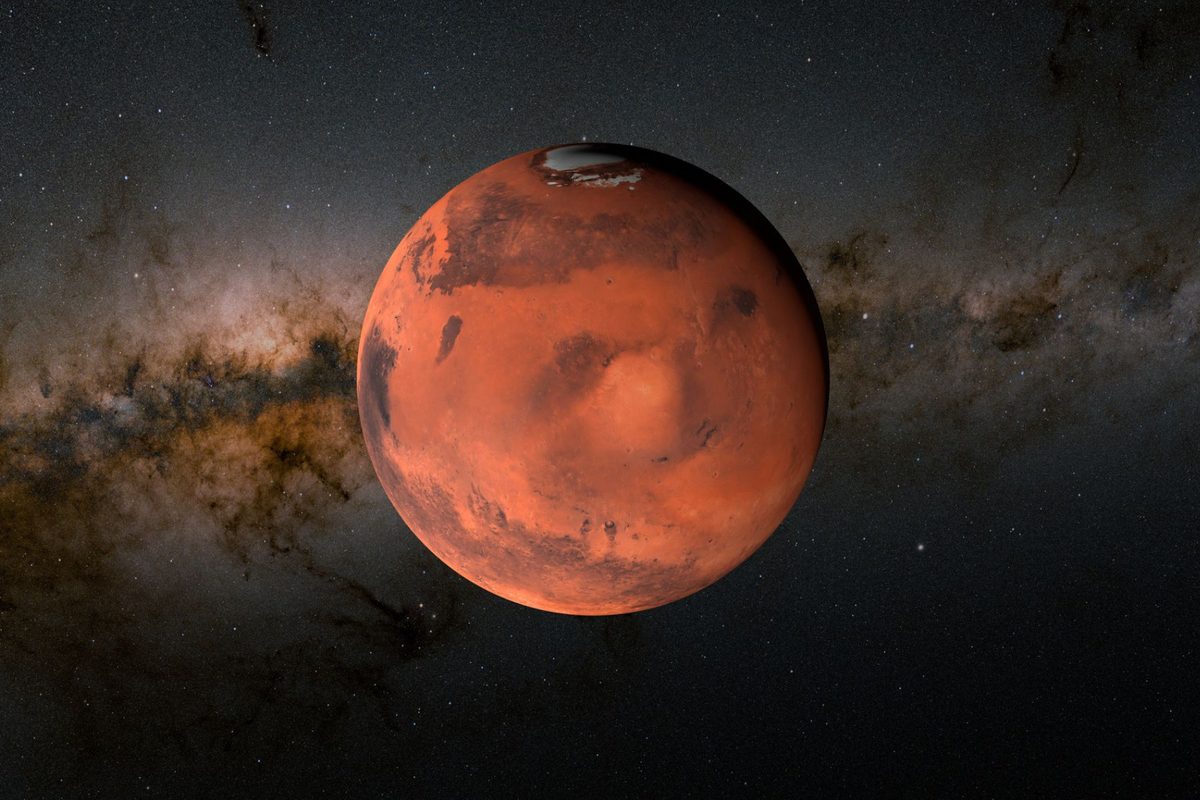
One of the most recognisable features of Mars is its red colour. Even the naked eye can clearly discern the Red Planet’s ruddy hue.
Humans have wondered where this red colour comes from for centuries, perhaps millennia.
Previously, it was…

Every year, TechCrunch’s Startup Battlefield pitch contest draws thousands of applicants. We whittle those applications down to the top 200 contenders, and of them, the top 20 compete on the big stage to become the winner, taking home the…

“Wrinkle” has been…

Unlock the Editor’s Digest for free
Roula Khalaf, Editor of the FT, selects her favourite stories in this weekly newsletter.
US retail chain Target is facing pressure from an activist investor after a sales slump that has wiped out nearly a third of its share value this year, according to people familiar with the details.
Toms Capital Investment Management, a US hedge fund that built a stake in Tylenol maker Kenvue before its $48.7bn sale to Kimberly-Clark last month, has made a significant investment in Target, the people said. The exact size of TCIM’s stake is unknown.
The pressure comes after Target in November reported its 12th consecutive quarter of negative or negligible sales growth.
Target’s share price has fallen more than 60 per cent from its all-time high during the Covid-19 pandemic, when customers flocked to it as a one-stop shop for necessities, clothes and home goods. It has underperformed the wider retail sector.
TCIM declined to comment. Founded by alumni of London-based hedge fund GLG Partners in 2017, it has recently built stakes and pushed for strategic changes at Pringles maker Kellanova, US Steel and Kenvue.
Shares in Target rose as much as 3.7 per cent on Friday after the Financial Times report on TCIM’s stake, giving the company a market value of $44.3bn.
Target said in a statement that it maintained a “regular dialogue” with all of its shareholders.
“Target’s top priority is getting back to growth, and our strategy to do so is rooted in three strategic priorities: leading with merchandising authority, providing a consistently elevated shopping experience and leveraging technology,” the company said. “We are confident the execution of this plan will drive the business forward and deliver sustained, long-term value for shareholders.”
Target’s longtime chief executive Brian Cornell plans to step down in February after more than a decade in the top job. He is being replaced by chief operating officer Michael Fiddelke, who after 23 years at the retailer has been tasked with orchestrating a major overhaul.
Fiddelke told investors last month that Target would spend $5bn in 2026, roughly $1bn more than this year, on improvements such as store renovations, product refreshes and a better digital experience. “We are not satisfied with our current results and are relentless in our pursuit of returning to growth,” he said on November’s investor call.
Analysts have highlighted Target’s advantages: 75 per cent of the US population live within 10 miles of its nearly 2,000 stores, second only to Walmart, and it owns 78 per cent of its stores. A recent UBS analyst report noted how Target could monetise its real estate in a similar way to US farm supply retailer Tractor Supply.
Yet consumers have become more cautious about spending, and Target, which relies more on discretionary goods such as decor, has been hit harder than rivals. Walmart’s share price is close to a record high, giving it a market capitalisation of almost $900bn, while the share price of warehouse club store Costco has more than doubled over the past five years.
In October, Target cut 1,000 roles and a further 800 open positions at its headquarters in Minneapolis, Minnesota. The job losses accounted for about 8 per cent of its 22,000 corporate employees.
With about half of its merchandise sourced from outside the US — China is its main source of imported products — it has been hit by US President Donald Trump’s sweeping tariffs.
While the tariffs have increased the cost of merchandise, Target lowered prices for 3,000 household essentials during the holiday shopping season.

Apple $AAPL ( ▲ 0.53% ) CarPlay’s popularity with drivers might not be enough to save the fate of the tech system as more automakers seek to retain control of their dashboards.
The details: Questions about the future of the in-vehicle…
A much-hyped novel about a housewife who uses Tupperware parties to secretly smuggle erotic stories to her friends and neighbours is causing a stir in the television world, igniting a fierce bidding contest over the right to adapt it for the…

You already know that your Amazon Prime membership is great for free two-day shipping. But what about all the other perks? Whether you’re prepping for New Year’s Eve festivities on a budget, or just trying to save some cash as the holidays wind…
