- Security forces kill nine Khwarij in Khyber Pakhtunkhwa RADIO PAKISTAN
- Security forces neutralise 9 terrorists in two separate KP operations: ISPR Dawn
- Soldier, 11 militants killed in two operations in northwest Pakistan Arab News PK
- Abbasi…
Author: admin
-
Security forces kill nine Khwarij in Khyber Pakhtunkhwa – RADIO PAKISTAN
-

The #1 Anti-Inflammatory Ingredient to Add to Your Soup
- Ginger adds flavor and natural anti-inflammatory compounds to soups.
- Fresh, powdered or lightly sweetened ginger can all work in savory recipes.
- Adding ginger to soups is an easy way to reduce inflammation.
When we think about the perfect…
Continue Reading
-

Hidden seismic signals hint at a tsunami threat in Alaska
Since 2020, scientists have installed monitoring instruments around the Barry Landslide in Alaska’s Prince William Sound to closely track seismic activity in the area. Their goal is to detect warning signs early, before a sudden landslide could…
Continue Reading
-
Security forces neutralise 9 terrorists in two separate KP operations: ISPR – Dawn
- Security forces neutralise 9 terrorists in two separate KP operations: ISPR Dawn
- Nine Khawarij neutralized in DI Khan, Bannu operations: ISPR Pakistan Today
- Nine terrorists killed in two separate KP operations: ISPR Geo News
- Nation stands united…
Continue Reading
-
Stereophonics phone box in Cwmaman has ‘likely been scrapped’, says BT
Having had various upgrades during its lifetime – including new glass, paintwork and signage – the payphone was one of several to have been earmarked for removal across RCT in 2019.
According to BT’s records, it had only been used 13 times in the…
Continue Reading
-
Stereophonics phone box in Cwmaman has ‘likely been scrapped’, says BT
 Getty Images
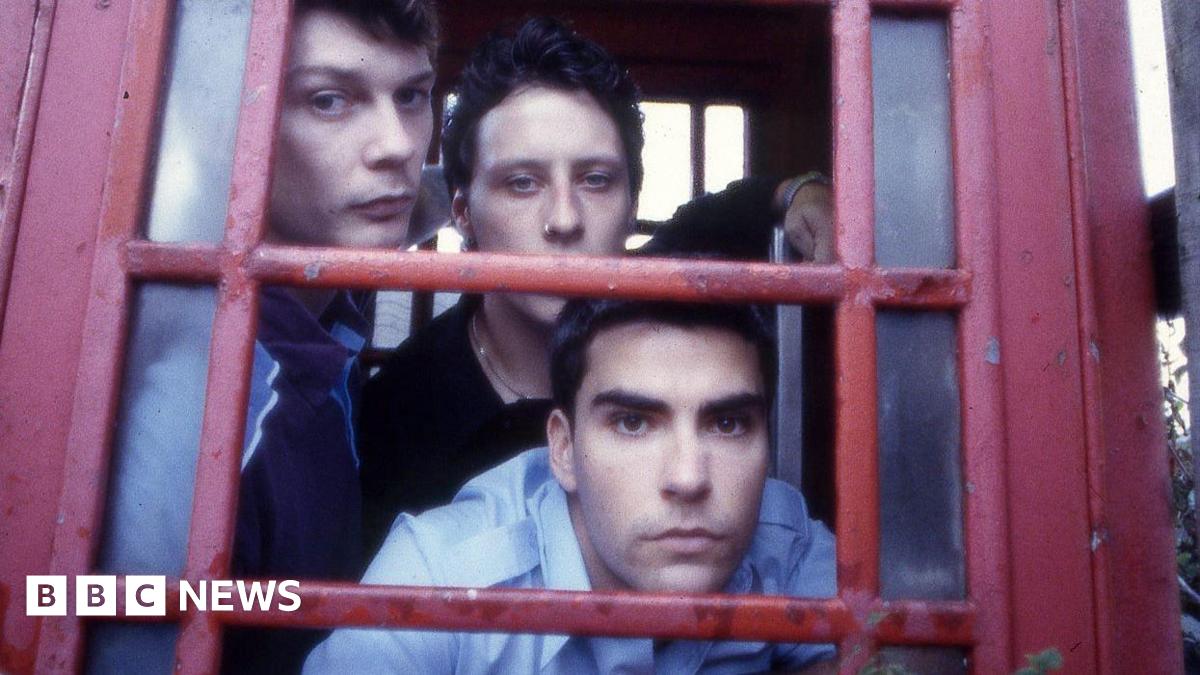
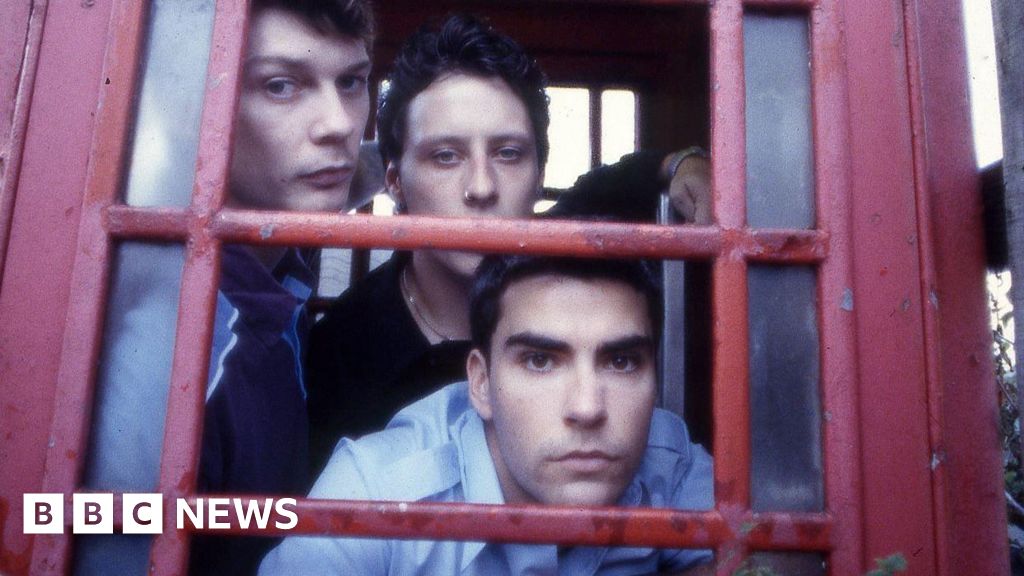
Getty ImagesThe original Stereophonics line-up pictured in the former Fforchaman Road phone box in 1997 A south Wales phone box made famous by rock group Stereophonics has “likely been scrapped”, telecoms firm BT has revealed.
The red kiosk in the…
Continue Reading
-

EA investigates after ‘foam’ reported on Birmingham river
The Environment Agency has said it is investigating after concerns were raised about possible pollution in a river in Birmingham.
Residents in the Selly Park and Stirchley areas shared concerns and photos on social media about “foam” seen travelling along the River Rea.
Pictures were taken in various locations, including alongside Cannon Hill Park, near the Rea Valley Cycle Path and near the city’s Third Avenue.
“We are aware of this incident and our officers are investigating,” said an agency spokesperson.
Continue Reading
-

EA investigates after ‘foam’ reported on Birmingham river
The Environment Agency has said it is investigating after concerns were raised about possible pollution in a river in Birmingham.
Residents in the Selly Park and Stirchley areas shared concerns and photos on social media about “foam” seen…
Continue Reading
-

The Earliest Known Plague Wasn’t Spread by Rats, DNA Study Reveals
For thousands of years, a prehistoric plague moved across Eurasia with terrifying efficiency. Scientists found its traces in human remains scattered far apart long before the Black Death gave the plague its grim reputation. What puzzled experts…
Continue Reading
-

Hidden holiday heart risks: Why heart attacks spike during the festive season
LOS ANGELES — As we indulge in heavier food and alcohol at this time of the year, there’s a hidden holiday danger we should be aware of.
Mix in a little stress, and it may add up to something called “holiday heart syndrome,” which usually refers…
Continue Reading