Kraków, Poland (March 6, 2026) – Based on the web series by The Unearthly Guy, Angel Engine is available on Steam today for $7.99. Developed by Black Lantern Collective and HMS Studios, and published by NerveLabs, the video game…
Author: admin
-
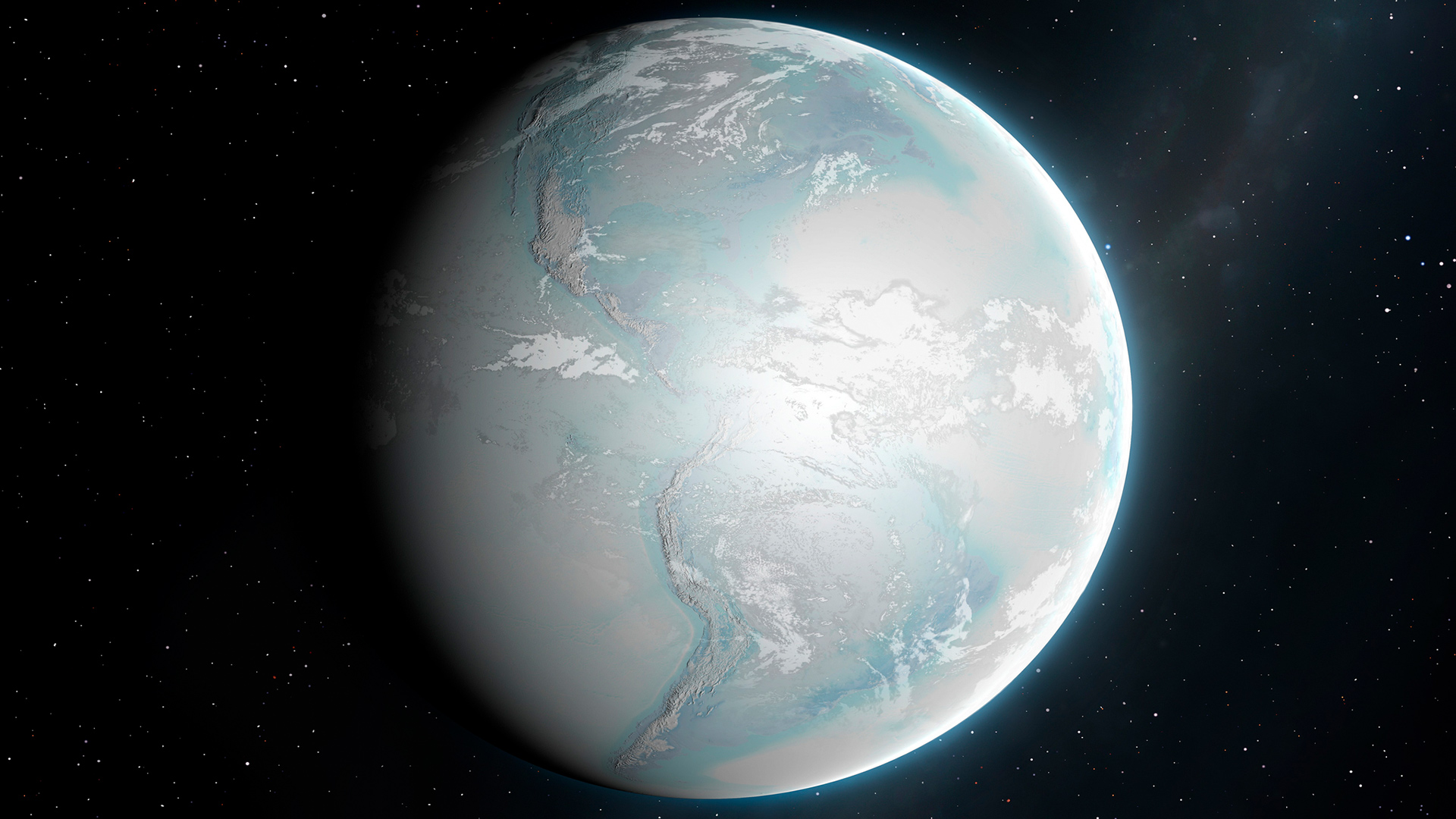
New model hints sea ice salt amplified Earth’s ancient global glaciation
Between 720 million and 635 million years ago, Earth may have experienced one of the most extreme climate episodes in its history. During this time, known as Snowball Earth, ice sheets are thought to have spread from the poles all the way to the…
Continue Reading
-

Forever Twilight? Satellite Mirrors Could Create Artificial Daylight From Orbit, Impeding Astronomical Observations
If a future catastrophe were to wipe out our civilization from the Earth’s surface, would there be a technological relic that would survive intact for billions of years?
One form of such relics would be satellites…
Continue Reading
-

PM seeks austerity, savings strategy to tackle global economic pressures
Prime Minister Shehbaz Sharif chairs federal cabinet meeting in Islamabad, February 18, 2025. — PID - Committee asked to submit recommendations within 48 hours.
- KP enforces fuel conservation, suspends non-essential…
Continue Reading
-
Taylor Swift confirms new single ‘Elizabeth Taylor’ after Easter Eggs
Taylor Swift fans excited for ‘Elizabeth Taylor’ release amid Selena Gomez collab rumours Taylor Swift has finally confirmed her next single as Elizabeth Taylor, after Swifties saw it coming from a mile away.
The…
Continue Reading
-

Lily Collins Recovers Her Engagement Ring Three Years After It Was Stolen
Losing your engagement ring is a very real nightmare—maybe it slips off of your finger, or you leave it on the side of a public restroom sink. Or, like Lily Collins, you experience the horror that is having it stolen. But there’s some cause…
Continue Reading
-
Efficient cardiac MRI multi-structure segmentation for cardiovascular assessment with limited annotation by integrating data-level and network-level consistency
Elliott, P. M. et al. 2014 ESC guidelines on diagnosis and management of hypertrophic cardiomyopathy. Kardiol. Polska 72, 1054–1126 (2014)..
Lalande, A. et al. Deep learning methods for automatic evaluation of delayed enhancement-MRI. The…
Continue Reading
-

F1 drivers eviscerate new cars at Australian GP – what’s going wrong, and is there a quick fix?
MELBOURNE, Australia — Formula 1’s controversial new cars didn’t just fail to pass their first audition, they fell flat on their face at the first yell of “action.”
The opening qualifying session of a brand-new regulation era in Melbourne should…
Continue Reading
-
Iran’s army vows to sink “enemy ships” entering the Gulf — media -Xinhua
TEHRAN, March 7 (Xinhua) — An Iranian military spokesperson said Saturday that “enemy ships” entering the Gulf will “end up at the bottom” of the waterway, according to multiple media reports.
Meanwhile, in a statement published on its…
Continue Reading
-

UAE ‘not an easy target’, President warns enemies against misjudging strength – Gulf News
- UAE ‘not an easy target’, President warns enemies against misjudging strength Gulf News
- UAE president says prepared to confront ‘threats’ as Iran attacks continue Al Jazeera
- Watch: UAE President visits victims of recent attacks receiving…
Continue Reading