Northwestern University engineers have developed the first haptic device that achieves “human resolution” – meaning it accurately matches the sensing abilities of the human fingertip.
Called VoxeLite, the ultra-thin,…

Northwestern University engineers have developed the first haptic device that achieves “human resolution” – meaning it accurately matches the sensing abilities of the human fingertip.
Called VoxeLite, the ultra-thin,…

A new review published in Frontiers in Science is calling for urgent action to avoid irreversible ecological damage by stemming the tide of microplastics entering the environment.
Climate change conditions turn plastics into more…

What drives a materials scientist to push the boundaries of what’s possible? We sat down with Yong Cui, one of our Materials Horizons editors, to explore not just the cutting-edge developments shaping the field, but the passion and…

The Lusail International Circuit awaits for the penultimate round of the 2025 season, with it playing host to the last Sprint event of the year.
Our duo head into this second round of the season-ending triple header on the back of mixed fortunes…
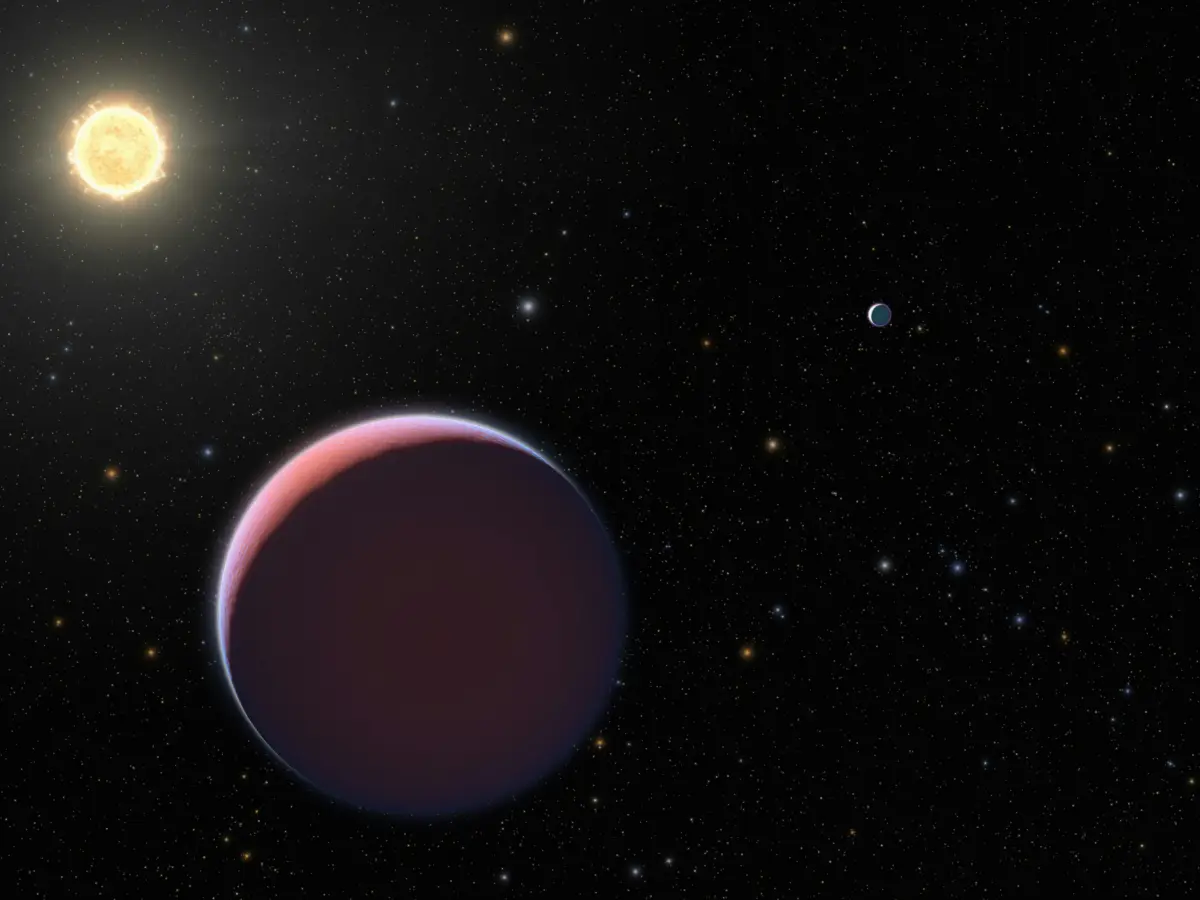
Scientists have found why Kepler-56, a red giant star, has a weird spin, and according to a new study, this is because it likely gobbled up one of the planets orbiting it. Takato Tokuno, a doctoral student in the Department of Astronomy at the…

The worst heartbreak and most riveting triumph of Anne Rice’s life happened in relatively quick succession, each beginning when the US novelist’s daughter – Michele, then about three – told her she was too tired to play.
Rice had never…