- Police detain protesters heading to Karachi Press Club for TTAP’s protest against 27th Amendment Dawn
- 27th Amendment protest blocked outside Karachi Press Club The Express Tribune
- Sindh Home Minister condemns attack on lawyers in Sukkur, orders…
Author: admin
-
Police detain protesters heading to Karachi Press Club for TTAP’s protest against 27th Amendment – Dawn
-
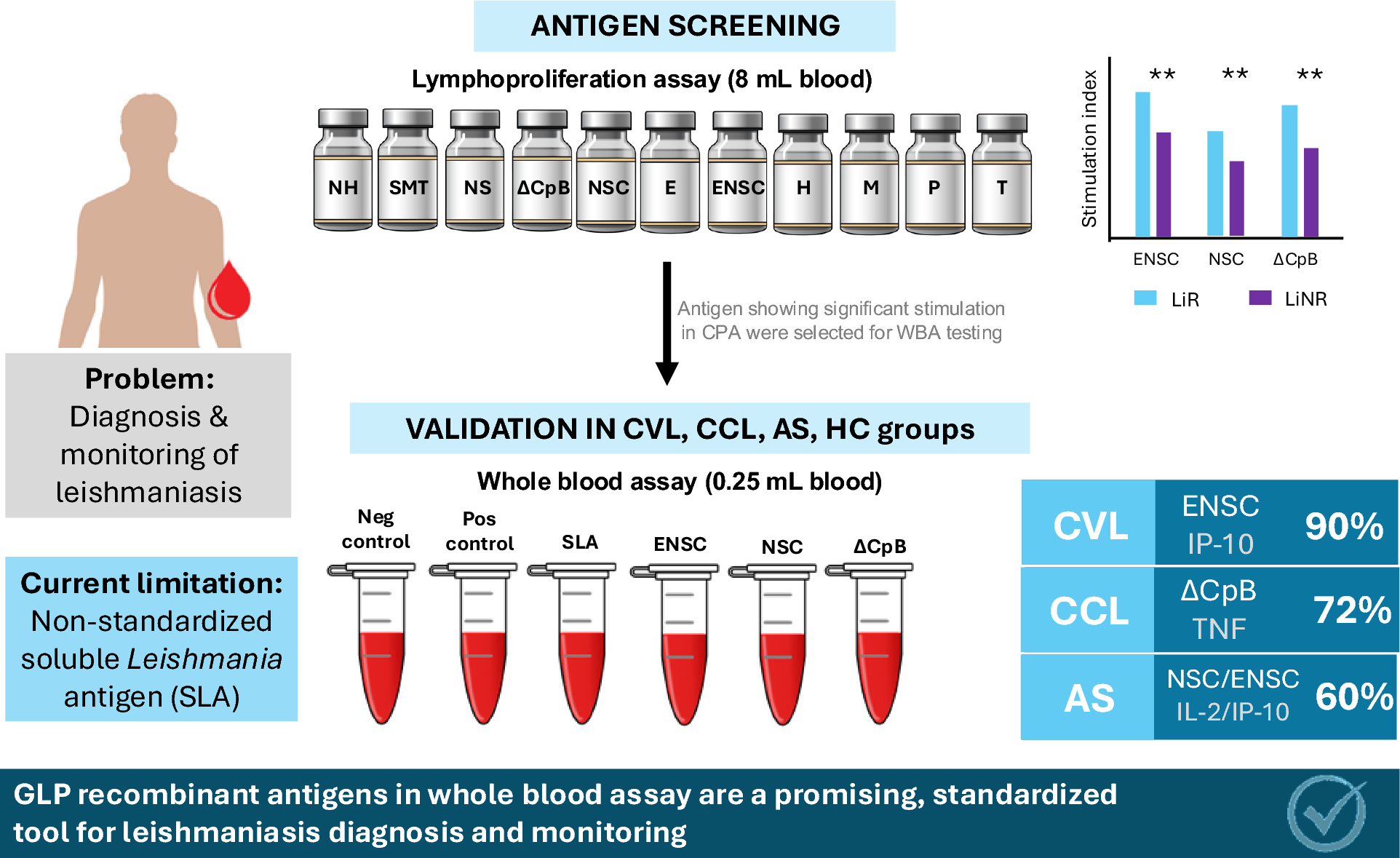
Diagnostic potential of GLP recombinant antigens in whole blood assays for Leishmania infantum infection | Parasites & Vectors
Ruiz-Postigo JA, Grouta L, Jain S. Global leishmaniasis surveillance, 2017–2018, and first report on 5 additional indicators. Wkl Epidemiol Rec WHO. 2020;25:265–80.
Singh OP, Hasker E, Sacks D,…
Continue Reading
-

Jimmy Kimmel accuses Trump of trying to get him fired and tells him: ‘Quiet, piggy’ | US news
Early on Thursday morning, Donald Trump made another plea for ABC to fire the late-night comedian Jimmy Kimmel, writing on his Truth Social platform that he has “NO TALENT” and “VERY POOR TELEVISION RATINGS”.
On his show later that night,…
Continue Reading
-
Statement by the Spokesperson
On several media queries soliciting Pakistan’s comment on the sentence awarded in the trial of the Former Prime Minister of Bangladesh, the Spokesperson stated the following:
This is an internal matter of…
Continue Reading
-

Two thirds of women gain ‘too much or too little’ weight in pregnancy – Nursing Times
- Two thirds of women gain ‘too much or too little’ weight in pregnancy Nursing Times
- Two thirds of women experience too much or too little weight gain in pregnancy BMJ Group
- Why weight during pregnancy has a big impact on both mums and…
Continue Reading
-
Scientists Recreate Conditions from the First Moments After the Big Bang – Hungary Today
- Scientists Recreate Conditions from the First Moments After the Big Bang Hungary Today
- UIC scientists recreate the universe’s first moments by slamming together oxygen ions UIC today
- STAR Pinpoints Quark-Gluon Plasma Phase Transition…
Continue Reading
-
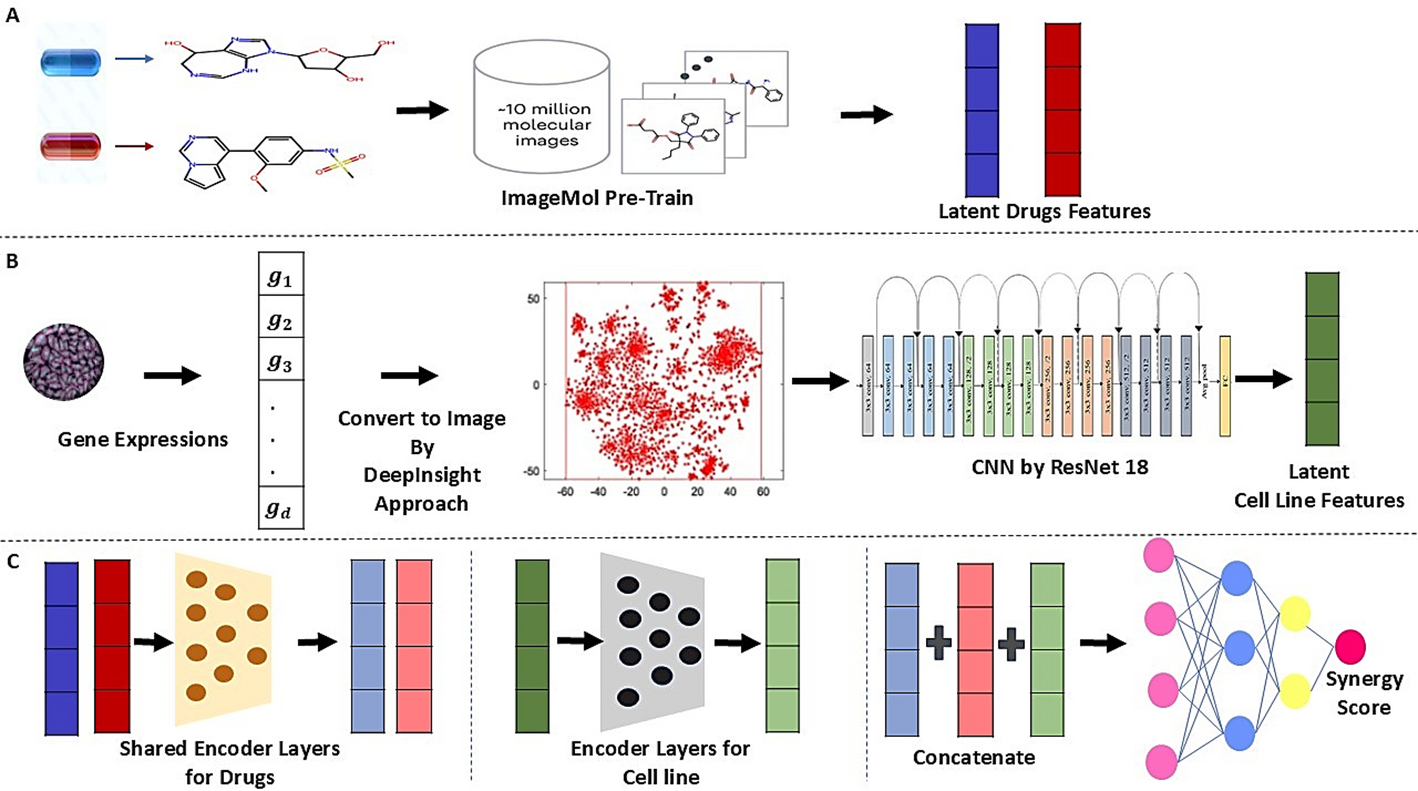
SynergyImage: image-based model for drug combinations synergy score prediction | BMC Bioinformatics
Overview of SynergyImage
The SynergyImage model consists of three steps for predicting drug synergy scores.
-
i.
Image-based features related to each drug are…
Continue Reading
-
i.
-
Best of the Week: Coverage of the EAS Conference, Detecting Lunar Water Ice
This week, Spectroscopy published a variety of articles highlighting recent studies in several application areas. Key techniques highlighted in these articles include nuclear magnetic resonance (NMR), visible and near-infrared (VNIR)…
Continue Reading
-

Mahira Khan breaks down in tears in Dubai as Fawad Khan opens up about struggles: ‘It hasn’t been easy’
Dubai: What made Mahira Khan cry in Dubai? Not exhaustion. Not travel chaos. Not the wrong, old passport in hand. Not the whirlwind Neelofar promotions.
She cried because her Humsafar co-star Fawad Khan — normally guarded, composed, and famously…
Continue Reading
-
Spinning into the merging binary black hole family tree – Astrobites
- Spinning into the merging binary black hole family tree Astrobites
- The Most Massive Black Hole Merger Ever Seen Was So Rare, It Seemed Impossible. Now, Astrophysicists May Finally Have an Explanation Smithsonian Magazine
- Twin Black Hole…
Continue Reading