
ISLAMABAD: Pakistan will consider a ceasefire with Afghanistan “over” even if a single cross-border attack occurred inside Pakistan, the Pakistani military said on Monday, with the two sides due to meet again in Istanbul this…
Author: admin
-

Canada-Pakistan Joint Statement: Reaffirming strong and enduring ties
November 3, 2025 – Ottawa, Ontario – Global Affairs Canada
Today, Honourable Anita Anand, Minister of Foreign Affairs, and His Excellency, Senator Mohammad Ishaq Dar, Deputy Prime Minister and Foreign Minister of Pakistan, issued this…
Continue Reading
-
Just a moment…
Just a moment… This request seems a bit unusual, so we need to confirm that you’re human. Please press and hold the button until it turns completely green. Thank you for your cooperation!
Continue Reading
-
UK Regulator Targets Delays in Rare Disease Treatments – Medscape
- UK Regulator Targets Delays in Rare Disease Treatments Medscape
- Major change for rare disease treatments on way, signals MHRA GOV.UK
- MHRA set to overhaul the UK’s rare disease drug regulatory pathway European Pharmaceutical Review
- New drugs to be approved faster so patients don’t wait years The Times
- MHRA reforms will speed up path for rare therapies Healthcare Management Magazine
Continue Reading
-
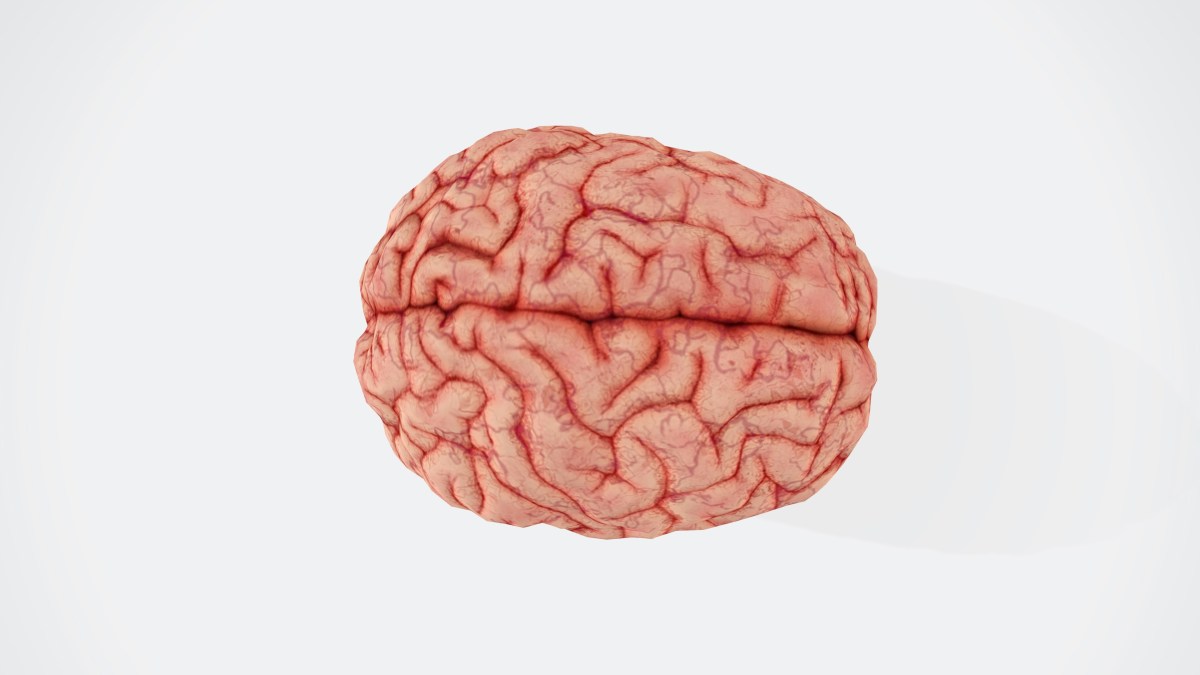
Form of brain cancer found to dissolve skull – The Tartan
By Amy Ji and Qinglin Kong
Glioblastoma is considered the most aggressive form of brain cancer. Courtesy of BUDDHI Kumar SHRESTHA via Unsplash Glioblastoma (GBM) is the kind of diagnosis no one wants to receive. It’s the most aggressive…
Continue Reading
-
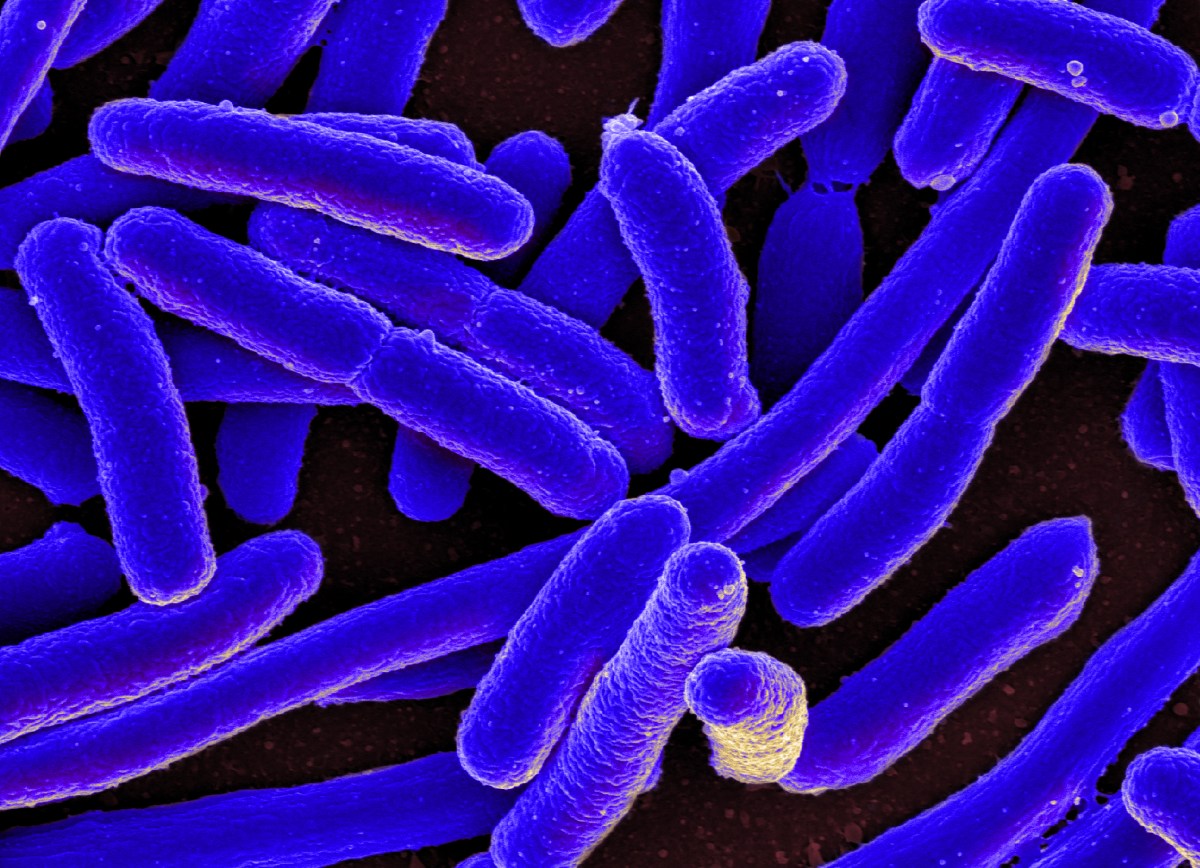
WHO reports increase in antibiotic resistance – The Tartan
E. coli bacteria, such as those pictured, are growing resistant to antibiotics with 40 percent of E. coli currently resistant to the preferred antibiotic treatment. “E. coli bacteria,” by NIAID from Wikimedia Commons under CC BY… Continue Reading
-

Pakistan’ s ceasefire with Afghanistan will be ‘over’ if cross-border attacks continue — military
ISLAMABAD: Pakistan will consider a ceasefire with Afghanistan “over” even if a single cross-border attack occurred inside Pakistan, the Pakistani military said on Monday, with the two sides due to meet again in Istanbul this…
Continue Reading
-

All About Equine Asthma: Causes, Signs and Management
Asthma isn’t just a condition in people — it affects horses, too. In fact, equine asthma is one of the most common chronic respiratory problems veterinarians see. It can impact any horse, from backyard companions to elite athletes, and ranges…
Continue Reading
-
Apple Invites UK to Express Creativity on iPad This Christmas with Drawing Competition – Little Black Book | LBBOnline
- Apple Invites UK to Express Creativity on iPad This Christmas with Drawing Competition Little Black Book | LBBOnline
- Apple invites the UK to participate in Your Tree on Battersea and express creativity on iPad this Christmas Apple
- Apple launches…
Continue Reading
