…

Spain’s King Felipe VI will pay a state visit to China from November 10 to 13, marking the first visit by a Spanish monarch in nearly two decades. The visit comes as both Madrid and Beijing look to strengthen bilateral trade, investment, and…

The Punjab government has intensified its anti-smog campaign as a thick haze continues to shroud Lahore and its surrounding districts. With air quality levels declining daily, authorities have launched a province-wide enforcement drive targeting…
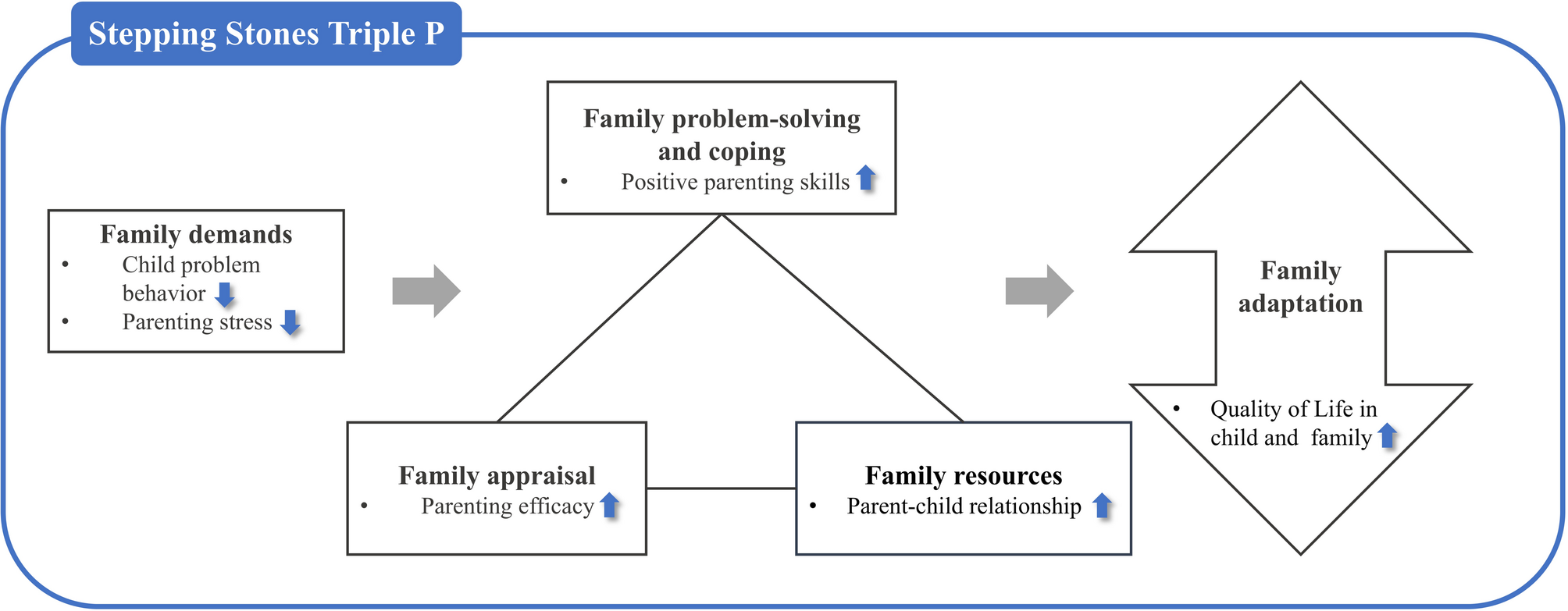
To our knowledge, our pilot study is the first attempt to conduct Level 4 Group SSTP among South Korean families. We adapted the Group SSTP to South Korean families of children with DDs and evaluated the intervention’s feasibility and effectiveness on the child and family outcomes based on the Resiliency Model [22].
Participants expressed high satisfaction with the intervention, indicating its potential in South Korea. They valued learning practical parenting skills and sharing insights with peers, with some expressing a desire to maintain connections after the sessions. While remote sessions eased participation for some, others preferred in-person meetings, suggesting that future research could offer both options. Overall, the feedback confirmed the intervention’s feasibility.
However, attrition was a potential consideration in assessing the feasibility, as two parents withdrew early. One, a single mother of a child with significant behavioral challenges, discontinued after the first session due to difficulty managing her child during the session, noting the absence of caregiving support. Another mother missed several sessions due to personal reasons, without attributing her non-participation to dissatisfaction with the intervention or difficulties with the virtual format.
Compared to traditional in-person delivery, the virtual format improved accessibility, enabling parents from distant regions to participate in real time. Nevertheless, the absence of a controlled physical environment may have introduced distractions that affected retention. The challenges experienced by the caregiver may have resulted from the combination of the specific characteristics of this intervention with its online delivery format, rather than the modality alone. For example, the parent might have more readily participated in an online program that actively engaged the child, thereby reducing the cognitive and logistical demands of attending to both the session and the child simultaneously. This highlights the need to assess not only the feasibility of the delivery modality in isolation but also the feasibility of the entire intervention package within its implementation context. Future research should explore strategies such as providing additional support for childcare or incorporating content that actively engages children.
In terms of individual-level score trends, Subject 6 demonstrated the most positive changes in all outcomes, except for the child’s problem behavior, across the time points (T0–T2). The baseline scores for the outcomes were relatively unfavorable, and the mother was young and had a lower economic status. She expressed a desire to participate in an additional round of the intervention, as she found it particularly helpful in learning parenting strategies tailored to her child. This participant did not report prior intervention experience, which may help explain the notable improvements observed. On the other hand, Subject 2 exhibited the least favorable outcomes, including declines in parenting efficacy, positive parenting skills, and family QoL. Notably, this participant’s baseline scores were relatively high, and her economic status was comparatively more favorable than that of other participants. The differences between the two subjects may stem from disparities in opportunities to participate in various interventions, influenced by their differing socioeconomic statuses. These patterns, though based on a small sample, highlight the importance of considering caregiver background and tailoring program outreach and delivery to reach underserved populations who may benefit most. Thus, future studies should investigate caregivers’ backgrounds, including prior intervention experiences with various delivery modalities such as virtual formats, to better understand how these may influence participation and engagement. Moreover, as in other countries where SSTP is implemented nationally [26], adopting the program at a national level in South Korea may be particularly beneficial for underserved families who lack access to parenting resources.
Additionally, although Subject 2 reported a high level of satisfaction with the intervention and provided positive qualitative feedback, she rated the usability and usefulness of the mobile app the lowest among all participants and expressed difficulties with app usage. Conversely, Subject 7, who reported the second-highest ratings for the usability and usefulness of the mobile app, demonstrated the greatest reduction in the child’s behavioral problems. This may suggest that the mobile app functioned as a supplementary tool in delivering the intervention, and its seamless integration into the intervention process could enhance overall effectiveness.
In terms of group level, we observed that comparisons between T0 and immediately post-intervention (T1) showed no statistically significant differences. However, we found significant effects of the intervention on child and family outcomes, including children’s behavior problems, QoL, parenting stress, efficacy, positive parenting behavior, and the parent-child relationship, from pre-intervention to one month post-intervention (T2).
One possible explanation for these findings is the cumulative effects of the intervention. SSTP focuses on providing families with practical parenting strategies that align with their values and needs, aiming to empower them to manage challenges independently [23]. Even after the intervention, families continued to apply positive parenting skills, which may have contributed to the improved outcomes observed over time.
The main limitation of our study was its small sample size. Therefore, our findings should be interpreted with caution. The outcome data gathered only from participant reports may have had a self-report bias. Including other informants may provide a more balanced assessment of the intervention.
Teede HJ, Tay CT, Laven J, Dokras A, Moran LJ, Piltonen TT, et al. International PCOS network. Recommendations from the 2023 international Evidence-based guideline for the assessment and management of polycystic ovary syndrome. Fertil Steril….

– Advertisement –
DERA ISMAIL KHAN, Nov 03 (APP):The Rescue 1122 Dera Ismail Khan organized a dengue prevention and awareness campaign to educate citizens about protective measures against the mosquito-borne disease.
The campaign aimed to…
This multi-national population-based cohort study presents routinely collected data from Danish, English, and Swedish patient registries and electronic health records that were linked to national statistics in each country.
We extracted individual participant data from the Danish National Patient Registry (DNPR), Hospital Episode Statistics Admitted Patient Care database (HES APC) for England, and from the Swedish National Patient Register (SNPR) [12,13,14]. For simplicity, the term registry will be used in the following for all three countries.
The DNPR includes data from all Danish hospitals, both public and private, covering inpatient care and, since 1995, also including outpatient care. It captures information such as diagnoses, surgical procedures, treatments, complications, and hospital admissions. The DNPR also records information on outpatient visits to specialist clinics and emergency department visits [12]. After identifying the Danish study population in the DNPR, it was linked to the Civil Registration System (CRS) by the unique 10-digit personal identification number given to all Danes at birth or immigration since 1968. This allows individual-level linkage of data between multiple registries. The CRS also contains information on date of birth, age, sex, and vital status [17].
HES APC is a dataset containing data on all remunerated activity within National Health Service hospitals (NHS) or NHS-funded care in England where the patient requires an inpatient stay in secondary care. This includes day-case procedures and provides data on primary and secondary clinical diagnoses. Data can be linked at a patient level to all other secondary care episodes within the NHS, in addition to national mortality data [14].
The SNPR contains information from inpatient care and, since 2001, also from outpatient care, thus including hospital admissions, emergency department visits, and specialist outpatient visits. It covers data from all Swedish hospitals, both public and private, and includes information on patient demographics, diagnoses, treatments, and procedures [13]. To ensure a high degree of completeness from the SNPR, the Swedish data extract did not include data from before 2001.
Information about the specific content of each national patient registry is provided in Table S1 (Additional file 1: Table S1) [12,13,14, 17,18,19,20,21]. Furthermore, population data for incidence calculation were extracted from national statistics in each country [18, 20, 21]. All individual-level data were provided in a de-identified format.
Based on the International Classification of Diseases, 10th Revision (ICD-10), all adults (≥ 18 years) with PHF (S.42.2*) were identified in the three national patient datasets [11,12,13].
The participants’ first fracture on each arm was included. In cases where laterality codes were missing, only the first fracture in one arm was included. Each index episode was analysed as an independent observation.
The exclusion criteria included the presence of bilateral PHF, any concurrent injury, and cancer registered at the same episode/index date as the fracture. This was to exclude polytrauma and pathological fractures. Specific details of the ICD-10 codes used for including and excluding patients, as well as recording comorbidities and SAEs, are found in Table S2 (Additional file 1: Table S2-S4).
The primary outcome variables were the numbers of pre-defined surgical procedures for PHF. The Nordic Medico-Statistical Committee (NOMESCO) Classification codes (NCSP-codes) were used to identify surgical procedures linked to the ICD-10 code in Denmark and Sweden, while Operational Procedure Codes, 4th Edition (OPCS-4) were used to identify surgical procedures linked to the ICD-10 code in England [19, 22]. The predefined surgical procedures were: plate fixation, screw fixation, K-wire fixation, intramedullary nail (IM nail) fixation, external fixation, and arthroplasty. If patients had surgery within 30 days after the fracture index date, surgery was considered as initial treatment. If the index date of the surgical procedure was later than 30 days after the fracture, the initial treatment was categorised as non-operative, thus, they were excluded from the analysis. A complete coding list for the surgical procedures can be found in Table S2 (Additional file 1: Table S2). If more than one surgical procedure was performed on the same date and no data were available to classify which was the primary, the procedure was classified using a predefined hierarchy (Additional file 1: Table S5).
Each specific surgical procedure was linked to the first episode of each SAE in a set of SAEs, occurring within 30 days after the index date of the surgical procedure. The SAEs were identified based on ICD-10 codes and included: stroke, respiratory tract infection, myocardial infarction, pulmonary embolus, urinary tract infection, and acute renal failure. In addition, mortality within 30 and 90 days was counted.
To identify potential confounding, age, sex, and comorbidities were compared between surgical subgroups and between countries. Information on history of ischaemic heart disease (IHD), diabetes mellitus (DM), and chronic obstructive pulmonary disease (COPD) was extracted. The overall level of comorbidity was calculated as the CCI using the algorithm by Quan et al. [23]. In Denmark and Sweden, a one-year lookback period was applied when extracting past medical history and CCI variables, whereas in England, no time limit was applied to the lookback period due to the limitation of no outpatient and emergency department information within the English dataset.
The primary investigators, responsible for the data in each participating country, cleaned and processed their national data. Data management flow charts for each country can be found in supplementary material (Additional file 2: Fig. S1a,b,c). Patient-level analyses were performed securely according to locally agreed data management procedures. Do-files were developed and shared among the three countries to enable reproducible analytical pipelines in each centre.
National baseline characteristics of patients divided by surgical subtype after isolated PHF were presented to identify potential differences in population profiles and sources of bias.
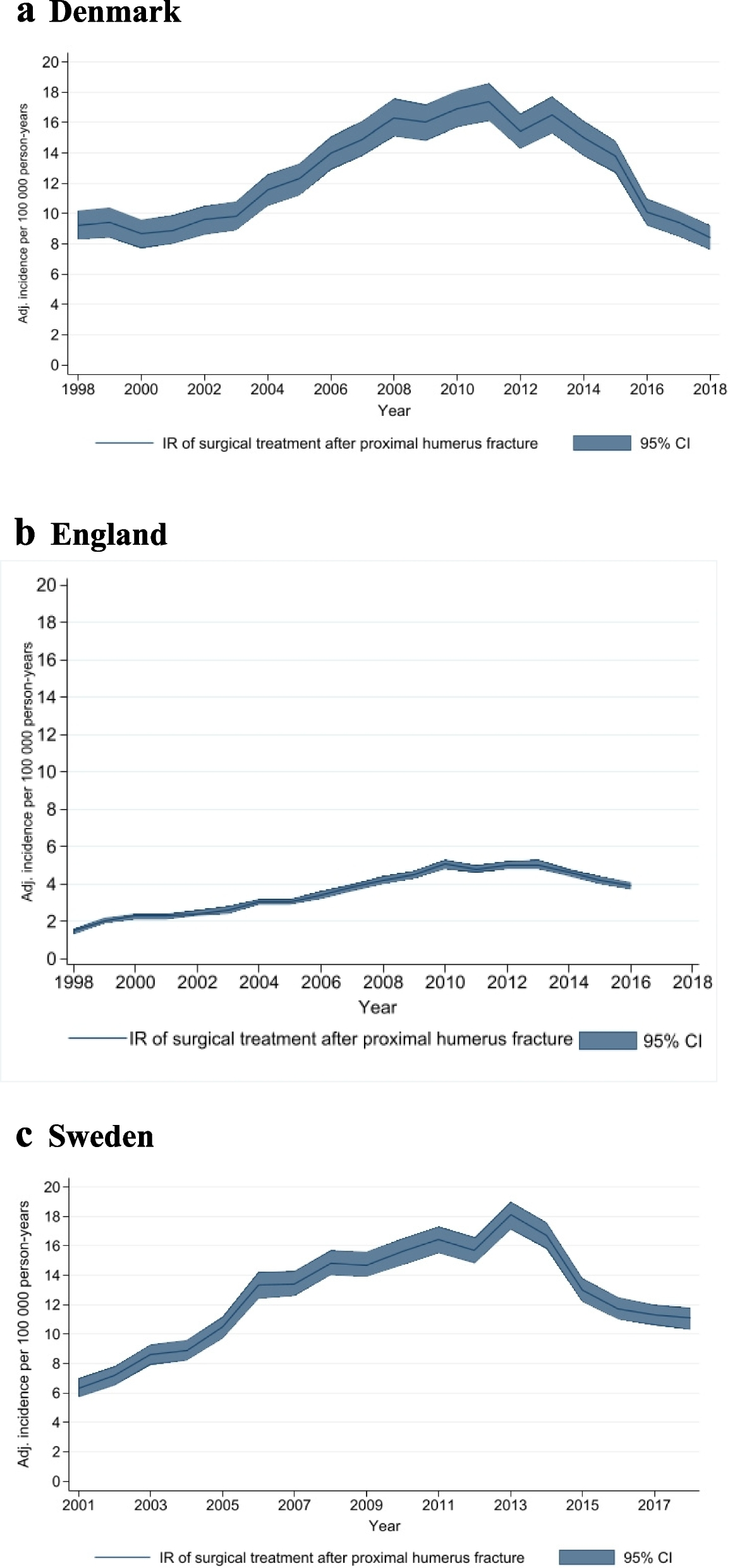
For each country, incidence rates (IR) per 100,000 person-years with 95% confidence intervals (95% CI) were calculated for all surgically managed PHFs and for each surgical subtype. This was done by using national population estimates. In addition, age- and sex-specific IRs were calculated. The annual surgical IRs for all three countries were plotted against the date of a Cochrane systematic review and a large clinical trial, to determine if there was an impact of trial recruitment or publication of high-quality evidence [9, 10].
SAEs, occurring within 30 days of each surgical procedure, were presented as cumulative incidence proportions (hereafter referred to as incidence) with 95% CI, assuming a normal approximation to the Poisson distribution for random count data.
Survival analysis using a Kaplan–Meier method was undertaken to show survival over the first post-operative year, as well as for the entire study period. Patients were censored at the date of death or end of follow-up, whichever came first.
Multivariable logistic regression analysis was undertaken to determine the impact of age (in 20-year age bands), sex, and overall comorbidity (using CCI categorised as (0–1), (2–3), (4 +)) upon the rise of SAEs within 30 days as well as 30-day, 90-day, and 1-year post-operative mortality.
Aggregated results from each country were compiled by the first author. The statistical package Stata (version 17, StataCorp, College Station, TX) was used for data cleaning, pre-processing, and statistical analyses.
The study was reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement [24].