- S&P Global Adds Hubert Joly to its Board of Directors S&P Global
- S&P Global Appoints Hubert Joly as New Director TipRanks
- S&P Global appoints former Best Buy CEO Hubert Joly to board Investing.com
- S&P Global Appoints Hubert Joly to the Board of Directors and Member of Audit and Compensation and Leadership Development Committees, Effective January 2, 2026 marketscreener.com
Category: 3. Business
-
S&P Global Adds Hubert Joly to its Board of Directors – S&P Global
-
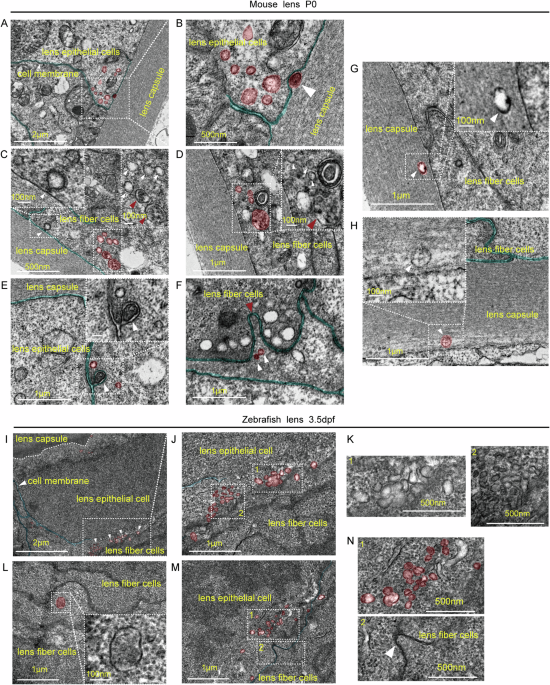
In vivo imaging reveals exosome-mediated intercellular communication in lens development
Zebrafish strains
Zebrafish were raised and cared for following standard protocols57. Wild-type AB zebrafish were maintained and bred in the fish facility at the Zhongshan School of Medicine, Sun Yat-sen University, Guangzhou, adhering to local animal welfare guidelines. The fish were kept at a controlled temperature of 28.5 °C and fed a diet of live and pellet food. Zebrafish embryos were collected through natural spawning and staged according to hours post-fertilization (hpf) or days post-fertilization (dpf). All experimental procedures were approved by the local ethical review committee of the Zhongshan School of Medicine, Sun Yat-sen University.
Construction of pCS2(+)-Cd63-AcGFP
To construct the pCS2(+)-cryaa promoter, the CMV IE94 promoter in the pCS2+ plasmid (#CZP1, CZRC, Hubei, China) was replaced with the cryaa promoter25. Then, Cd63-AcGFP (cd63: National Center for Biotechnology Information, NM_199543) and AcGFP were synthesized and cloned into the pCS2(+)-cryaa promoter, respectively. The cryaa promoter, Cd63-AcGFP, and AcGFP were synthesized by GENEWIZ (Jiangsu, China). To induce lens-specific expression of Cd63-AcGFP, embryos were injected with the plasmid at the one-cell stage. The following day, the embryos were examined under a stereomicroscope. Embryos that were dead or had developmental abnormalities were removed, and only those with a normal appearance were retained for further analysis.
Morpholino injection
Morpholinos (denoted by “MO” below) were purchased from Gene Tools (Philomath, USA). Syntenin-a-MO was adopted from a previously published study22. The sequence is: 5′-TACAACGACATCCTTTCTGCTTTCA-3′. The sequence of standard control morpholino is 5′- CCTCTTACCTCAGTTACAATTTATA-3′. Different doses of MO, including 2, 4, and 8 ng/nl, were injected for testing. To minimize the potential off-target effects, 2 ng/nl of ctrl MO or 2 ng/nl of Syntenin-a-MO was used. Real-time PCR was used to verify the knockdown efficiency. The primers used are listed in Supplementary information: Table S1.
Construction of pCS2(+)-Syntenin-a-DsRed
For the rescue experiments, morpholino-insensitive Syntenin-a–DsRed and DsRed were synthesized by GENEWIZ (Jiangsu, China) and individually cloned downstream of the cryaa promoter in the pCS2(+) vector. Zebrafish embryos at the one-cell stage were co-injected with pCS2(+)-Cd63-AcGFP, either Ctrl MO or SyntA MO, and either cryaa–Syntenin-a–DsRed or cryaa–DsRed, yielding four groups: Ctrl MO + OE-Ctrl (cryaa–DsRed), Ctrl MO + OE-Exp (cryaa–Syntenin-a–DsRed), SyntA MO + OE-Ctrl (cryaa–DsRed), and SyntA MO + OE-Exp (cryaa–Syntenin-a–DsRed). The following steps are as described above.
Live fluorescence imaging
At 24 hpf, PTU (200 µM) was added to the embryo-rearing water to inhibit melanin production. At 48 hpf, the zebrafish were anesthetized with tricaine (0.016%) and embedded in 1.5% low-melting-point agarose for positioning. After positioning at the lens, 3D images with a z-stack and time series videos were captured via a ZEISS LSM980 confocal microscope, and the images were reconstructed and analyzed using ZEN software (3.1).
Transmission electron microscopy (TEM)
Lens from 3.5 dpf zebrafish and postnatal (P) 0 mice were collected and transferred into TEM fixative (G1102, Servicebio, Hubei, China) for 2 h at room temperature (RT) and another 24 h at 4 °C. The samples were subsequently dehydrated at RT, penetrated with resin, embedded, and polymerized. After positioning, ultrathin sections were cut and stained with 2% uranium acetate and 2.6% lead citrate. Finally, the sections were examined and imaged via a TEM (JEM-1400Flash, Rigaku, Japan).
Immunoelectron microscopy (IEM)
Zebrafish embryos injected with the cryaa-Cd63-AcGFP plasmid at 3.5 dpf were fixed in IEM fixative (G1124, Servicebio). The samples were washed 3 times with prechilled 0.1 M PBS (pH 7.4) in an ice box. After dehydration in a gradient of prechilled alcohol, resin infiltration, embedding, polymerization, and ultrathin sectioning, the sections were subjected to immunogold labeling. In brief, after being blocked with 1% BSA at RT for 30 min, the sections were incubated with an anti-GFP antibody (A-11122, Thermo Fisher, Massachusetts, USA) at 4 °C overnight. GFP antibody was subjected to immunogold labeling with PAG 10 (G7402, Sigma, Missouri, USA) the next day. After uranium counterstaining, the sections were observed and imaged via a TEM.
EVs isolation from zebrafish embryos (ZF-EVs)
One hundred zebrafish embryos injected with the cryaa-Cd63-AcGFP plasmid at 3.5 dpf were anesthetized according to welfare standards, the rearing water was removed, and the embryos were washed 3 times with Ringer’s solution (containing 116 mM NaCl, 2.9 mM KCl, and 5.0 mM HEPES). During this process, the sample was intermittently blown with a sterile 200 µl tip to completely remove the yolk syncytial layer. The embryos were subsequently placed in a 35 mm petri dish with 2 ml of 0.25% trypsin/ 1 mM EDTA at 37 °C for digestion. During this period, the embryos were blown with a sterile 200 µl tip every 10 min until the digestion was complete, which ensured that no large cell clumps or tissue blocks were visible. The entire process took approximately 30–45 min. CaCl2 (1 mM) and 10% fetal bovine serum (FBS, Biowest, Nord, France) in PBS were used to stop trypsin activity. The final volume was transferred to centrifuge tubes. Differential centrifugation at 300 × g (2 × 10 min), 1200 × g (2 × 10 min), and 10,000 × g (1 × 60 min) was performed to eliminate cellular debris. The supernatant was filtered through a 0.22 μm filter and then centrifuged at 100,000 × g (2 × 90 min). The pellet was resuspended in PBS and stored at −80 °C until use.
The morphology of the ZF-EVs was evaluated via TEM. Fifty (50) micrograms of ZF-EVs were diluted (1:40) with PBS, and then the diluted EVs suspension (20 μL) was dropped onto a 300-mesh cell strainer and incubated for 10 min. Excess liquid was absorbed with filter paper, and the samples were counterstained with 1% phosphotungstic acid for 30 s and observed under a TEM. Nanoparticle tracking analysis (NTA, NanoSight NS300, Malvern, United Kingdom) was used to determine the particle number and size distribution of the ZF-EVs.
Nanoflow cytometry
EVs Membrane Red Stain dye (NEPU-638, NanoFCM, Fujian, China) was diluted with PBS to prepare a 100× working solution. One μL of the diluted 100× working solution was added to 99 μL of EVs sample at a concentration of 2 ~ 6 × 108 particles/ml. The mixture was mixed thoroughly and incubated at 37 °C for 15–20 min in the dark. Detection and analysis were subsequently performed via nanoflow cytometry using a Flow Nano Analyzer (U30E, NanoFCM, Fujian, China) equipped with three lasers (405, 488, and 640 nm wavelengths).
Human embryonic stem cells (hESCs) culture
The H1 hESCs line was kindly provided by Professor Shuyi Chen at the Zhongshan Ophthalmic Center. Mycoplasma contamination was routinely checked using a PCR-based assay to ensure the cell lines were free of contamination. The cells were cultured on plates coated with growth factor-reduced Matrigel matrix (354277, Corning, New York, USA) in mTeSR1 medium (# 85850, STEMCELL Technologies, Vancouver, Canada) without feeder cells. For maintenance, the cells were plated in 6-well plates at 37 °C, 5% CO2, and the culture medium was changed daily. The cells were passaged with Gentle Cell Dissociation Reagent (# 100-0485, STEMCELL Technologies, Vancouver, Canada).
Lentoid body induction
When the density of the H1 cells reached approximately 80–90%, the culture medium was replaced with lentoid body induction culture medium according to the protocol51. The basal medium used for lentoid body induction was Dulbecco’s modified Eagle’s medium/F-12 (C11330500BT, Gibco, Waltham, MA, USA) supplemented with 1% minimum essential medium nonessential amino acid solution (11140050, Gibco), 2 mM GlutaMAX (35050061, Gibco), 0.05% BSA (199897, MP Biomedicals, Ohio, USA), N-2 supplement (17502048, Thermo Fisher Scientific, Waltham, MA, USA), and B-27 supplement (17504044, Thermo Fisher Scientific). Growth factors were then added sequentially to the medium as follows: 100 ng/mL Noggin (120-10C-20, PeproTech, New Jersey, USA) from Days 0 to 6 (stage 1), 100 ng/mL FGF2 (100-18B‒100, PeproTech) and 20 ng/mL BMP4 (120-05‒5, PeproTech)/BMP7 (120-03 P‒10, PeproTech) from Days 7 to 18 (stage 2), and 100 ng/mL FGF2 and 20 ng/mL Wnt3a (315-20‒10, PeproTech) from Days 19 to 35 (stage 3). The culture medium was replaced every other day. For EVs treatment, 50 μl of 0.5 μg/μl ROR1-EVs was added to the medium from days 20 to 35. The lentoid bodies were photographed via a Zeiss Axio Observer Z1 microscope (Zeiss, San Diego, CA, USA) on Day 35 and were collected for further analysis.
Magnetic-activated cell sorting
A magnetic-activated cell sorting (MACS) method was used to purify ROR1+ cells32. First, we prepared single-cell suspensions using TrypLE (Thermo Fisher Scientific) on Day 30 of lentoid induction. Next, an Anti-ROR1 MicroBead Kit (130-103-929, Miltenyi Biotec, Bergisch Gladbach, Germany) was used to label the cells, which were sorted with a MACS cell separator (130-042-201, Miltenyi Biotec). The resulting ROR1+ cells were plated on Matrigel-coated culture plates in M199 medium (Thermo Fisher Scientific) containing 10 ng/ml FGF2 (100-18B-100, Peprotech), 10 ng/ml IGF1 (100-11-100, PeproTech, New Jersey, USA), 10 μg/ml insulin (HY-P0035, MedChemExpress, New Jersey, USA) and 0.05% BSA (199897, MP Biomedicals, Ohio, USA). The culture medium was replaced every other day. To analyze the purity of the ROR1+ cells, we performed flow cytometry using an ROR1 antibody (357806, Biolegend, California, USA). ROR1+ cells from passages 0 to 3 were used for the experiments. To induce the differentiation of ROR1+ cells, the maintenance medium was switched to lentoid induction medium as mentioned above, supplemented with 100 ng/μL FGF and 20 ng/μL Wnt3a. After one-week, lentoid formation was observed, followed by examination of lens differentiation markers via immunofluorescence staining.
RNA-seq
Total RNA was extracted from ROR1+ cells using TRIzol reagent (15596-018; Thermo Fisher, USA). The analysis was performed with 3 biological replicates. The RNA was quantified via the K5500 system (Beijing Kaiao, China), and RNA integrity was assessed via the Agilent 2200 TapeStation (Agilent Technologies, USA). The sequencing libraries were generated via the NEBNext® Ultra™ II RNA Library Prep Kit for Illumina (#7775, NEB, USA) following the manufacturer’s instructions. The libraries were sequenced on the Illumina NovaSeq platforms (Illumina, USA) with 150 bp paired-end reads at RiboBio Co., Ltd. (Ribobio, Guangdong, China). After filtering, the clean reads were aligned to the human reference genome (GRCh38) via HISAT258. Then, feature counts were used to determine the number of reads mapped to each gene, and the transcripts per kilobase of exon model per million mapped reads (TPM) value was calculated for each gene. GO and KEGG functional enrichment analyses were performed via the DAVID59,60 (https://david.ncifcrf.gov/tools.jsp), followed by visualization using an online platform (https://www.bioinformatics.com.cn). Gene expression heatmap were performed using ComplexHeatmap packages (version 2.13.1).
Isolation of EVs from ROR1+ cells cultured in vitro
To isolate ROR1+ LPCs-EVs, the medium was collected after the cells were cultured for 48 h, and EVs were extracted via differential centrifugation. The supernatant was centrifuged sequentially at 300 × g for 10 min and 2000 × g for 30 min to remove cell debris. The resulting mixture was ultracentrifuged at 10,000 × g for 60 min and then filtered through a 0.22 μm filter. Next, we extracted EVs using ultracentrifugation (Optima XE 100 centrifuge) at 100,000 × g for 90 min, as described above. The final pellet was resuspended in PBS and stored at −80 °C until use. TEM, NTA, and WB were used to detect the morphology, particle number, and size distribution, and surface markers of the ROR1+ LPCs-EVs, respectively. The protein concentrations of the ROR1+ LPCs-EVs were measured using a BCA protein assay kit (A55864, Thermo Scientific, USA). The doses used in all subsequent experiments were based on the measured protein concentrations.
Western blot analysis (WB)
Lentoid bodies collected on Day 35 were lysed with RIPA buffer. The protein concentration was quantified via a BCA protein assay kit (A55864, Thermo Scientific, USA). The proteins were mixed with 5× SDS sample buffer, and equal amounts of protein were separated via sodium dodecyl-polyacrylamide gel electrophoresis (SDS‒PAGE). The proteins were then transferred onto polyvinylidene fluoride (PVDF) membranes via electroblotting. The membranes were blocked with 5% nonfat milk and incubated overnight at 4 °C with specific primary antibodies. After being washed with TBS containing 0.1% Tween 20 (TBST), the membranes were incubated with HRP-conjugated secondary antibodies. The target protein bands were detected using an enhanced chemiluminescence reagent (NcmECL Ultra, NCM Biotech, Suzhou, China) and a chemiluminescence detection system (ChemiDoc™ Touch, Bio-Rad Laboratories, California, USA). The antibodies used: PAX6 (1:1000, ab195045, Abcam, Cambridge, UK), αA-crystallin (1:500, sc-28306, Santa Cruz, Texas, USA), β-crystallin (1:200, sc-48335, Santa Cruz), γ-crystallin (1:200, sc-22746, Santa Cruz), and β-actin (1:1000, 4970, Cell Signaling Technology, Massachusetts, USA).
RNA isolation and quantification
Total RNA was extracted from cells using TRIzol reagent (15596-018; Thermo Fisher). Reverse transcription was performed using a PrimeScript RT Master Mix kit (TaKaRa, Kyoto, Japan), and quantitative PCR was performed using a SYBR Premix Ex Taq kit (TaKaRa, Japan) on a LightCycler 480 (Roche, Basel, Switzerland). GAPDH was used as an internal control. Relative gene expression was determined by the 2−ΔΔCt method. The primers used are listed in Supplementary information: Table S1.
Immunofluorescence staining
Zebrafish cryosections or cultured cells were fixed with 4% paraformaldehyde for 10 min at RT. After washing with PBST, the cryosections or cells were permeabilized with 0.5% Triton ×–100 for 10 min and blocked with 5% normal donkey serum for 30 min. Afterward, the sections or cells were incubated with different primary antibodies at 4 °C overnight in a humidified chamber. The next day, Alexa Fluor 488-conjugated or Alexa Fluor 568-conjugated secondary antibodies were applied, and the samples were incubated for 1 h at RT. After washing with PBST, the samples were counterstained with DAPI for nuclear staining. The samples were observed using an LSM980 confocal microscope or an inverted fluorescence microscope. The antibodies used: αA-crystallin (1:100, sc-28306, Santa Cruz), β-crystallin (1:100, sc-48335, Santa Cruz, Texas, USA), γ-crystallin (1:200, sc-22746, Santa Cruz), F-actin (1:200, C2201S, Beyotime, Shanghai, China), β-catenin (1:200, sc-7963, Santa Cruz), GFP (1:200, A-11122, Thermo Fisher, Massachusetts, USA), TOM20 (1:200, 11802-1-AP; Proteintech Group, Illinois, USA), LAMP1 (1:200, ab24170; Abcam, Cambridge, UK), PAX6 (1:300, ab195045, Abcam), Six3 (1:200, sc-398797, Santa Cruz), Sox2 (1:400, 23064, Cell Signaling Technology), and BMI1 (1:100, 5856S, Cell Signaling Technology).
Bromodeoxyuridine (BrdU) labeling and immunostaining
At 3.5 dpf, zebrafish embryos were positioned laterally in a drop of embryo medium for microinjection. A pulled glass capillary loaded with a 10 mM BrdU solution (Sigma-Aldrich) was used to deliver approximately 0.5 nL into the cardiac region adjacent to the caudal yolk sac. After a 2-h period in fresh water, embryos were fixed, permeabilized, and processed for immunofluorescence. Finally, incorporated BrdU was detected by incubating the specimens with a mouse anti-BrdU monoclonal antibody (1:300, RPN20, GE Healthcare) following standard immunofluorescence protocols.
Extracellular vesicle uptake assay
To monitor the internalization of ROR1+ LPCs-EVs, the isolated ROR1+ LPCs-EVs were labeled with DiI Cell-Labeling Solution (V22885, Thermo Fisher, USA). In brief, 100 μl of EVs were diluted to 1 ml with PBS, 10 μl of Dil was added to the suspension, and the mixture was incubated at 37 °C for 10 min. Subsequently, the mixed suspension was centrifuged at 100,000 × g for 60 min. After the supernatant was discarded, the pellet was resuspended in PBS to obtain Dil-labeled ROR1+ LPCs-EVs. Then, the labeled ROR1+ LPCs-EVs were added to a lentoid induction system, which was subsequently fixed and stained for immunofluorescence after 48 h of incubation. A ZEISS LSM980 confocal microscope was used to acquire fluorescence images.
Label-free mass spectrometry analysis
For label-free proteomic analysis, three biological replicates were prepared. The proteins in the ROR1+ LPCs-EVs samples were prepared and digested with trypsin. The resulting peptides were analyzed via liquid chromatography‒tandem mass spectrometry (LC‒MS/MS) using an UltiMate 3000 RSLCnano system coupled with a Q Exactive HF mass spectrometer through a Nanospray Flex ion source (Thermo). The MS data were analyzed using MaxQuant software (version 1.6.6) and searched against the human protein sequence database downloaded from UniProt. Proteins were identified and quantified, and the results were filtered with a 1% false discovery rate (FDR) at both the peptide and protein levels. Protein levels were normalized to the iBAQ values [%] for expression analysis. The total protein list for the ROR1+ LPCs-EVs was generated by identifying proteins that were simultaneously present in three samples (315 identified proteins). We utilized the DAVID bioinformatics resources to conduct GO and KEGG enrichment analyses. GSEA analysis was performed using gseGO and gseKEGG function of clusterprofiler R packages (version 4.4.4). The enrichment analysis results were visualized via https://www.bioinformatics.com.cn.
Statistical analysis
We performed statistical analysis using GraphPad Prism version 8.0 (GraphPad software). Student’s two-tailed t test was used for two-group comparisons. All quantitative data are shown as the mean ± standard deviation (SD). P value less than 0.05 was considered to indicate statistical significance.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Continue Reading
-

AP Business SummaryBrief at 7:47 a.m. EST – Citizen Tribune
- AP Business SummaryBrief at 7:47 a.m. EST Citizen Tribune
- US jobs report shows rise in unemployment BBC
- Payrolls rose by 64,000 in November after falling by 105,000 in October, delayed jobs numbers show CNBC
- Live Q&A: Ask WSJ Editors About the State of the Labor Market and the Economy The Wall Street Journal
- Nonfarm payrolls take a sharp downturn, signaling economic uncertainty By Investing.com Investing.com South Africa
Continue Reading
-

Coventry University Group on track to break even in this financial year
Coventry University Group is firmly on course to break even in this financial year after two years of reform as UK Higher Education continues to battle a financial crisis.
The Group identified in 2023 that it needed to reduce spending by £95million across a three-year programme of reshaping and resizing to establish a sustainable global education group. It said at the time that would include two years of planned deficits before recording a breakeven position in 2025/26.
Accounts for the year ending 31 July 2025 were published today showing a deficit for a second year, as predicted, alongside a steep reduction in costs of £39million compared to the previous year.
A major factor in the size of the deficit was due to the Group recruiting far more students than planned in spring 2025. The cost of recruiting those students sits in the 2024/25 accounts while most of the income sits in the 2025/26 accounts – skewing the financial picture.
That influx of students, which saw overall numbers grow year-on-year, is just one factor helping drive confidence in hitting the breakeven target in this current financial year.
In common with many in the sector, we have worked with the Office for Students (OfS), England’s Higher Education regulator, on a review of our financial strategy, governance and ability to deliver sustainability and the OfS has confirmed we currently do not need to continue to the further stage of review.
Professor John Latham CBE, Vice-Chancellor and CEO of Coventry University Group, said there is a high level of confidence that the Group transformation and its focus on global and national innovative delivery means it is back on an upward trajectory at a time when OfS expects 45% of universities to be in the red.
We were open and honest about how the sector problems would affect UK Higher Education and what we were going to do about it. The sector needed to reform and our teams have been incredible in their speed and agility to make the changes we needed happen.
The required deficits are never easy, but inevitable as the scale of reforms we have implemented are now having a positive impact on our finances. After the first quarter of this financial year, we are ahead of where we planned to be. Student numbers are bouncing back and we now have a structure which will allow us to pursue sustainable growth.
We still have substantial cash reserves and strong assets, which sends a strong and reassuring message to our stakeholders and the regulator
The OfS considers 24 providers to be financially at risk and could be forced to stop offering degree-awarding courses within the next 12 months. Our going concern statement demonstrates we are not in that unfortunate position, and our stakeholders can have confidence in our future.
We have brought forward a wide range of reforms to what we do and how we do it, while protecting our TEF Gold-rated teaching. All of our post-graduate teaching has successfully moved to block teaching and the first round of feedback from students has been overwhelmingly positive. We are now pushing ahead with implementing block teaching across all under-graduate courses from September 2026 and moving to six intakes a year.
This innovation in education was made in Coventry, successfully developed and delivered in our CU campuses in Coventry, Scarborough and London for more than 10 years and is now being widely copied across the country.
We won’t stop innovating, diversifying and finding new sources of income in the UK and global markets, using our teaching, research and knowledge transfer activities to continue creating better futures.
Everyone in Higher Education knows we operate in an uncertain sector with many challenges outside of our control. We are certain that we have the correct strategy and are on the right path.
Professor John Latham CBE, Vice-Chancellor and CEO of Coventry University Group
Coventry University Group is a global education group which includes Coventry University, Coventry University London, Coventry University Wroclaw in Poland, CU campuses in Coventry, Scarborough and London and the National institute of Teaching and Education, alongside branch and badged campuses around the world and a network of Global Hubs.
KEY FINANCIAL DATA
- Income: £380.1m
- Expenditure: £447.1m
- Deficit: £59.3m (pre tax)
- Staff costs: £222.7m
- Other operating expenses: £176.2m
- Amortisation and depreciation: £39m
- Tuition fee and education income: £303.8m
- VC bonus: 0
- Liquidity days: 90+
Continue Reading
-
Arrival of Universal comes one step closer as Government grants planning permission – Bedford Borough Council
- Arrival of Universal comes one step closer as Government grants planning permission Bedford Borough Council
- Universal Theme Park development gets the green light WhatsOnStage
- Universal Studios gets green light to be built in Bedfordshire BBC
- Breaking news: Green light given for Bedford Universal Studios theme park Bedford Independent
- It’s happening: Universal Studios gets green light after Government grants planning permission Bedford Today
Continue Reading
-
Week of Quality 2024 training kit
Overview
Ensuring quality of the health product ensures its safety and efficacy. Manufacturers in low-
and middle-income countries (LMICs) face challenges to achieve quality in local production,
such as the lack of an available manufacturing workforce trained in quality and understanding
regulatory quality standards and difficulties in implementing a quality culture in the
manufacturing facility.
The Local Production and Assistance (LPA) Unit in the Innovation and Emerging Technologies
Department (IET), Access to Medicines and Health Products Division (MHP), WHO, supports
Member States (MS), particularly LMICs, to strengthen sustainable local production and
technology transfer to improve timely, equitable access to quality, safe and effective essential
medical products.The LPA Unit provides assistance and support to MS with an ecosystem
wide and holistic approach, such as conducting ecosystem assessments for sustainable,
quality local production, developing and implementing strategies, roadmaps and tools,
providing comprehensive capacity building and technical assistance, including for WHO
Prequalification (PQ)/Emergency Use Listing (EUL), and facilitating technology transfer (TT).To support MS to overcome challenges to locally produce quality-assured vaccines and
biotherapeutics, medicines and in vitro diagnostics (IVDs), the LPA Unit organized a new
global training event – Week of Quality – to complement the annual Virtual cGMP Training
Marathons also organized by the LPA Unit. The first Week of Quality was organized from 16 to
20 June 2023 and focused on establishing quality specifications of vaccines, medicines and
IVDs based on WHO and other international guidelines, one of the stepping stones to
achieve quality.The second week of quality took place from 15 April to 13 June 2024 and
focused on exploring key aspect of regulatory compliance for Medicines, IVDs and Vaccines
and biotherapeutics. More than 1700 vaccine and biopharmaceutical manufacturers and
regulators attended the sessions on key aspects of vaccine and biotherapeutic
regulatory compliance. More than 1400 pharmaceutical manufacturers and
regulators strengthened their knowledge on quality requirements for pharmaceutical
product development. And for the first time, over 1000 IVD manufacturers and
regulators, built capacity in principles of design, quality and compliance for optimizing IVD
product development.Questions raised by manufacturers and regulators in the second Week of Quality have been
assembled in this training material with questions-and-answers (Q&A) with answers prepared
and peer-reviewed by experts with long and rich experience in the vaccine, medicine or IVD
industry, national regulatory authority (NRA), and other organizations. This document has
been developed to provide manufacturers and other relevant stakeholders with a continuous
learning resource and reference document to acquire new and fortify existing, knowledge
and capacities to strengthen the local production of quality vaccines, medicines and IVDs.Continue Reading
-

Trio of breaches spills data belonging to millions • The Register
Three very different companies have now confirmed data breaches affecting millions of users – each insisting the damage stopped well short of passwords and payment details.
Pornhub has told Premium subscribers that some user data was exposed after a breach at Mixpanel, a third-party analytics provider it once used, rather than through any compromise of Pornhub’s own systems.
In a notice to users, the adult site said the incident affected “only select Premium users” and involved a limited set of analytics events inside Mixpanel’s environment. Pornhub stressed that passwords, credentials, payment details, and government IDs were not exposed, and noted it stopped working with Mixpanel in 2021 but was informed of the breach by the vendor.
The disclosure follows a similar incident last week affecting OpenAI, which traced a leak of internal data to compromised Mixpanel analytics credentials.
SoundCloud has also confirmed it was breached after a week of user complaints about outages and broken access, which the company now says were linked to a cybersecurity incident. The streaming platform said it detected unauthorized activity in an ancillary service dashboard and brought in third-party security experts to investigate, eventually determining that the exposure affected roughly 20 percent of users.
According to public data, SoundCloud has approximately 140 million users, suggesting that some 28 million people have likely been affected by the breach.
According to SoundCloud, the data accessed was limited to email addresses and information already visible on public profiles, and did not include passwords or financial details. But the measures taken to contain the breach had side effects. Configuration changes introduced during the response caused “temporary connectivity issues” for some users, particularly those accessing the service via VPNs, effectively turning a behind-the-scenes security incident into a very public service disruption.
Over in Japan, retail giant Askul is still picking through the wreckage of an October ransomware attack that knocked systems offline and exposed customer data. In a new report [PDF], the office supplies and e-commerce giant said the incident caused “large-scale service stoppage” and confirmed that information it held “flowed outside the company” after its network was compromised.
In the report, translated by The Register, Akira Yoshioka, president and CEO of Askul, confirmed “the recent ransomware attack resulted in the leak of customer information, as well as the information of some of our business partners, and we apologize for the significant inconvenience and concern this has caused.”
Askul now says roughly 740,000 records linked to individual customers and corporate clients were affected, with some affected data published by the RansomHouse cybercrime crew, but says no financial details were accessed during the attack.
The lengthy report confirms that threat actors accessed Askul’s internal systems using the login details of a subcontractor “who exceptionally did not apply multi-factor authentication.” The firm also admits that the datacenter where the breach occurred “did not have EDR installed on its servers, nor was 24-hour monitoring performed, so unauthorized access and intrusion could not be detected immediately.”
Ransomware infection was confirmed in logistics and internal systems, and some data (including backups) was encrypted and rendered unusable. In addition, some of that data was stolen and leaked by the attacker.
Different sectors, different attackers, and very different root causes – but the same end result: user data escaping through analytics tools, ancillary systems, and ransomware-ridden networks, even as companies rush to reassure customers that the most sensitive details stayed put. ®
Continue Reading
-

Asda joins the team to help change lives through supported internships
A Hartlepool project creating life-changing opportunities for people with additional needs is going from strength to strength, with a retail giant now throwing its weight behind the scheme.
The Hartlepool Supported Internship Programme – a partnership between Hartlepool Borough Council, consultancy DFN Project Search and local employers – provides a structured, work-based learning programme to help young people aged 16-24 with additional needs and/or autism gain the skills, experience and confidence they need to move into paid employment.
The scheme has received another major boost after Asda Hartlepool joined the partnership – the first time the Hartlepool store has done anything like this.
Asda has welcomed nine young people into supported internships, with them each spending time learning the ropes in a range of different store areas including fresh and frozen food, George, health and beauty and general grocery items over a total nine month period.
As well as trying out different job roles in real working environments, the interns learn practical skills, timekeeping and communication, discover what kind of work they are good at and build their confidence and independence, all the time continuing with education and training and receiving support from job coaches and mentors.
From left: Councillor Aaron Roy, Rob Cecere of Asda Hartlepool, five of the supported interns – Aimee Mitchell, Joshua Grainger, Marc Phillips, Kieran Hunter and Noah Hunter – and Beth Madigan of DFN Project Search
Just a few weeks into their placements, the interns and Asda are already seeing major benefits.
Noah Hunter, who is 19, said: “I’m really enjoying it – it gives me a reason to come out of the house. It lets me do work and I’m really enjoying doing that.
“It’s made me more confident and has helped me improve my timekeeping. The staff in Asda are really nice and are always there if you need a helping hand.”
Aimee Mitchell, who is 20, said: “I am enjoying it – I feel good coming into work every morning and I’m proud of myself and happy, and I’m looking forward to the next few months.”
Councillor Aaron Roy, Vice-Chair of Hartlepool Borough Council’s Adult Services and Public Health Committee, said: “We were absolutely delighted to welcome Asda Hartlepool to the partnership – it’s testament to the confidence employers have in the Supported Internships scheme.
“For people with additional needs and/or autism, gaining and sustaining employment can often be far more difficult than for those who don’t have them, and these internships help change lives, building independence and confidence and showcasing the young people’s drive and determination.
“They are also good for business, increasing an employer’s confidence to develop employees with additional needs and increasing the diversity of the workforce, reflecting its customer base. We’d love more firms to follow Asda’s lead and come onboard.”
Rob Cecere, Asda Hartlepool General Store Manager, said: “Comparing how the interns were on day one when they first came in for the interviews with now just a few weeks later, we’ve already seen how they’ve grown, with their potential and passion shining through.
“We’re so excited to support this project and we’re really looking forward to the coming months and seeing how these young people continue to flourish.”
Beth Madigan, Programme Specialist for DFN Project Search, said: “We know that supported internships can change lives but we also know that it can really benefit a business and they can make use of an untapped talent pool.
“We’re really excited to see the ripple effect of this programme in Hartlepool, benefitting the community and raising aspirations for young adults with additional needs and/or autism and building a more inclusive workforce in the community.”
If you’re a Hartlepool business keen to get involved – or if you’re someone who would like to join one of the Supported Internships programmes – email SI@hartlepool.gov.uk
Continue Reading
-

Gold prices in Pakistan Today
At current prices, the looted gold is worth around $70 million. PHOTO: PIXABAY
Gold prices registered a sharp decline on Tuesday across both international and local markets.
In the international bullion market, spot gold fell 0.6% to $4,277.20 per ounce as of 1102 GMT, after earlier trading around $4,285. Despite the dip, bullion has rallied 64% so far this year.
Following the global downturn, gold prices in Pakistan also dropped sharply. The price of gold per tola declined by Rs4,000 to Rs450,862, while the price of 10 grams fell by Rs3,429 to Rs386,541.
Meanwhile, spot silver fell 1.5% to $62.98 per ounce, after touching a record high of $64.65 on Friday.
In the local market, silver prices remained unchanged, with the per tola rate steady at Rs6,532 and the price of 10 grams holding at Rs5,600.
Read: Gold records fresh gains as prices climb locally, internationally
Meanwhile yesterday, in the domestic market, gold per tola surged to Rs454,862, gaining Rs2,600 during the day. Similarly, 10-gram gold was sold at Rs389,970, up Rs2,229, according to the All-Pakistan Gems and Jewellers Sarafa Association.
On Saturday, the gold price per tola had closed at Rs452,262 following a decline of Rs2,000. Meanwhile, silver touched a historic high, rising Rs68 to reach Rs6,532 per tola.
Commenting on market trends, Adnan Agar, Director at Interactive Commodities, said that the gold market was not showing significant movement on Monday, trading between $4,300 and $4,350, with the rate later standing at $4,322.
“Key US economic data is scheduled to be released this week, including inflation and employment figures, as well as the Bank of Japan’s monetary policy decision. These events are likely to influence gold and overall financial markets,” he mentioned.
Agar added that gold was about $60-70 below its all-time high, while silver had already touched a record high. “Barring any unfavourable news, the overall outlook for gold remains positive,” he said.
Continue Reading
-

Glasgow Prestwick Airport: economic impact assessment
Economic Impact Assessment of Glasgow Prestwick Airport. On behalf of the Scottish Government Final Report: January 2025
Scottish Ministers
The Scottish Government St Andrews House
2 Regent Road Edinburgh
Dear Sirs / Madams,
Please find attached the Economic Impact Assessment of the Glasgow Prestwick Airport (“the Report”), shared by PwC UK with the Scottish Government (“SG”) in January 2025, in accordance with our agreement dated 20 December 2023. This Report has been prepared based on data shared by SG and Glasgow Prestwick Airport (“GPA”) during the period of March – December 2024. This report has been prepared in connection with the scope as set out in the engagement letter.
You have asked us to estimate the economic impact assessment of GPA to the Scottish economy, both from a Gross Value Added (“GVA”) and employment perspective using the latest available data. In conjunction to this, you have asked us to analyse the airport’s wider impacts, helping you determine the wider services being delivered by the airport. This has included data shared via case studies on 11 businesses and organisations in and around GPA.
As described in the agreement or as expressly agreed by us in writing, we accept no liability (including for negligence) to anyone else or for any other purpose in connection with this report.
Yours faithfully,
Simon Oates
PricewaterhouseCoopers LLP
Continue Reading

