JPMorgan is growing more bullish on Circle and stablecoins in general. The bank double upgraded the stablecoin issuer to overweight from underweight. Analyst Kenneth Worthington also lifted his price target to $100 from $94, implying upside of 16% from here. Shares of Circle have soared 178% since their IPO price of $31. The stock debuted on the New York Stock Exchange in June . However, Circle has plunged 67% from its June highs, opening a buying opportunity, Worthington wrote. CRCL YTD mountain CRCL YTD chart “With Circle’s share price under pressure in recent weeks in advance of a substantial lockup expiration, Circle’s stock price has approached and fallen below our previous Dec. 2026 price target ($94),” he wrote. “With enough upside in the shares for the stock to outperform our broader coverage universe and with key fundamentals improving, we raise our earnings estimates.” Worthington’s upgrade follows Circle’s “solid” third-quarter report, in which the company posted earnings and revenue that beat the Street. Still, the company fell 12% on Wednesday as operating expenses guidance for the year came in higher than expected as well. “The quarterly results indicate to us that stablecoins are continuing to make their way into mainstream financial services, with USDC a leading stablecoin and Circle a leading partner,” he wrote. “We also see that Circle is bringing more USDC on-platform, which will enable Circle to continue to boost growth while allowing it to more heavily invest in the buildout of its network.” Circle shares rose more than 1% following the double upgrade.
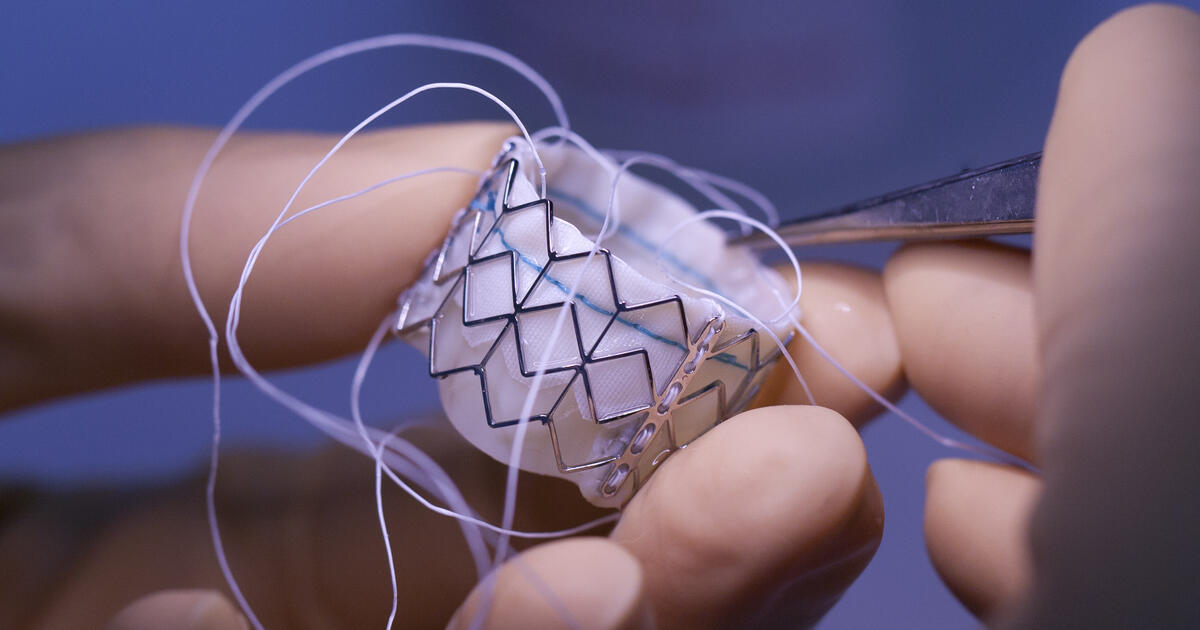
The Paris Central Division of the Unified Patent Court (UPC) ruled (40-page / 1.68MB PDF) that companies in the Meril Life Sciences group (Meril) infringed a European patent relating to a prosthetic heart valve and a delivery assembly. The patent, a third-generation divisional patent, belongs to US-based Edwards Lifesciences Corporation (Edwards). The patent was found to be valid as amended by an auxiliary request and the court granted an injunction prohibiting Meril from supplying a rival valve product in the UPC contracting member states in which the patent is in force. However, the injunction does not apply to all versions of Meril’s valve.
As Meril is the only manufacturer of an extra large version of the type of valve at issue, the Paris court considered there would be a public interest in exempting those versions of the product from the scope of the injunction. This is because it acknowledged that some patients who suffer from aortic stenosis – where the aortic valve into the heart is narrowed – and who would need an extra large valve to be implanted to address the condition could be left without an adequate treatment if those products were included within the scope of the injunction. The court reiterated that to rely on such a public interest defence, “it is essential to demonstrate that [it] is the sole available treatment method or that it represents an improvement upon a known treatment method, resulting in a notable enhancement in patient care”. The exemption in the present case only extends until such time as another equivalent treatment becomes available.
Sarah Taylor of Pinsent Masons, an expert in life sciences patent litigation, said the case provides lessons for businesses on both sides of a patent dispute.
“Injunctions remain an important remedy in a finding of infringement, but they may, in some circumstances, be limited for reasons of public interest,” Taylor said. “Businesses defending against an injunction should take the opportunity to narrow the reach of injunctions where there may be a real public interest reason for doing so. Those seeking injunctions should be aware that such relief may be limited where no alternative treatment method is available.”
The proceedings before the Paris court were initiated by Meril, as part of a long-running dispute between the parties. It asked the court to revoke Edwards’ patent, claiming that it was invalid for added matter, lack of novelty and lack of inventive step. Edwards filed an application to amend the patent and a counterclaim for infringement. After the parties had filed their written pleadings, Edwards requested, and was granted, leave to amend its counterclaim to explicitly extend it to cover Meril’s new heart valve product and delivery system. The court ultimately rejected Meril’s revocation action, maintained the patent as amended by an auxiliary request and upheld Edwards’ counterclaim for infringement.
In assessing the patent’s validity, the Paris court endorsed case law that the Munich Central Division developed last year on the question of inventive step.
Patents can only be obtained for inventions if those inventions are, among other things, new, not obvious, and have an industrial application. To pass the obviousness test, applicants must be able to show that their new product or process delivers an inventive step – i.e. there is a substantive technical advance that someone skilled in the relevant area would not be able to work out easily using their own know-how and information available to them.
Last year, in a case between Amgen on the one hand and Sanofi and Regeneron on the other, the Munich Central Division said that the question of whether there has been an inventive step taken should be assessed holistically.
The first step, it said, is to determine a “realistic starting point” in the prior art that would have been of interest to the skilled person considering a similar “underlying problem” as that which the patent claimed to solve. It said this ‘realistic starting point’ may be one of several and does not need to be the most promising starting point.
The next stage, the Munich court determined, is to ask whether it would be obvious for the skilled person to arrive at the claimed solution in the patent from the ”realistic starting point”. If the skilled person would be motivated to consider and implement the claimed solution in the patent as a next step, then the patent is obvious.
Taylor said the Paris court took the same approach in the Meril v Edwards case, confirming the need for a ”holistic” assessment, and highlighted guidance the court provided on what could constitute a ”realistic starting point” when assessing inventive step.
The court said: “A realistic starting point is a document ‘of interest’ for solving the objective problem. In this regard, it may be assumed that realistic starting points, in general, are the pieces of evidence which disclose the main relevant features as those of the challenged patent and for that reason have constituted the basis for the developing of the inventive idea and/or which address the same or a similar underlying problem.”
Taylor said, however, that the ”holistic approach” backed by the UPC in this case differs from the “problem-solution approach” used by the European Patent Office (EPO) to assess the question of inventive step, which requires the identification of the closest piece of prior art. It had been expected that the UPC would adopt this strict problem-solution approach, and while some divisions of the court have, others, including the Paris Central Division in this case, have deployed the holistic approach. UPC Court of Appeal clarification will ultimately be required to determine binding UPC case law on the issue, but Taylor noted that this difference could have “some implications for identifying the relevant starting point for solving the underlying problem and potentially any experts the parties may want to instruct”.
Taylor said, though, that the different approaches did not lead to a different outcome in the context of the dispute between Meril and Edwards, noting that Meril had lodged parallel opposition proceedings before the EPO before which its arguments pertaining to inventive step were also unsuccessful.
In the context of the parallel EPO proceedings, Taylor said it was noteworthy that the Paris court had exercised its discretion not to ‘stay’ its proceedings – that being, wait for the EPO proceedings to conclude before deciding the dispute before it.
“Clients with proceedings at the EPO and UPC should bear in mind the UPC’s discretion to stay/not stay proceedings,” Taylor said. “The bar to granting a stay is high, with the court keen to meet its aim of reaching a final decision within 12 to 14 months of proceedings being issued and willing to decide matters independently.”
In the present case, in exercising its discretion against a stay in this case, the Paris court considered the fact that neither party had requested a stay, which the court took as implicitly demonstrating the parties’ interest in a prompt decision by the court. Furthermore, at the time the Paris court was informed of the pending opposition proceedings before the EPO, the UPC proceedings were already at an advanced stage – the written phase had concluded, the interim conference had been held, and the oral hearing was imminent. The Paris court also observed that any stay of the proceedings would have the effect of postponing a decision in the infringement action, thereby frustrating Edwards’ interest in a swift protection of its exclusive right.
Taylor highlighted that it took Edwards less than a year from the point it extended its infringement counterclaim to obtaining an injunction against Meril from the Paris court, an injunction which also covers Meril’s new valve product. She said the speed at which the UPC can operate to grant patent rights holders such relief, and the front-loaded nature of UPC proceedings, is something businesses need to factor into their litigation and commercial strategy and planning.
“Parties should collate relevant information as early as possible to ensure written pleadings can be prepared and submitted in the short time frame,” Taylor said. “Additional evidence and information should be considered, collected and prepared early if a public interest defence may be brought into play. Thought should also be given to the approach the UPC may take to assessing inventive step, especially if there are also parallel opposition proceedings at the EPO – the identification of a ‘realistic starting point’ for solving the objective problem is important for the UPC, although it is debateable whether the two ‘different’ approaches are all that inconsistent.”
The European patent at issue in this case is part of a wider family of patents in the longstanding dispute between Edwards and Meril in relation to heart valves. Edwards was successful in pursuing infringement claims against Meril in relation to another of its patents relating to some of Meril’s heart valve products before the Munich Local Division of the UPC last year.
Milan, 12th November 2025 – Today, at the Godard Cinema of Fondazione Prada in Milan, the opening press conference of the “Joint International Conference 2025: Innovation in Oncology – New Drugs and the Impact of Artificial Intelligence” was held. The event is organized by Fondazione Gianni Bonadonna with the support of Prada Group, Fondazione Michelangelo, and the European School of Oncology. Scheduled for November 12–13, 2025, this international event brings together leading global experts in oncology – clinicians and researchers – for two intensive days dedicated to innovation in cancer research and care. The scientific program will address two major challenges in contemporary oncology research: on one hand, the latest frontiers in drug development and therapeutic strategies to overcome tumor resistance mechanisms; on the other, the growing impact of Artificial Intelligence in precision medicine. During the press conference, ongoing and future initiatives resulting from the collaboration between Fondazione Gianni Bonadonna and Prada Group were also presented, starting with the recent launch of the “Concerted Research Institute”. A central focus is also placed on training and empowering the next generation of researchers, with the announcement of the continuation of the “Gianni Bonadonna Fellowship”.
“Big Short” investor Michael Burry, known for his successful bets against the U.S. housing market in 2008, has deregistered his hedge fund, Scion Asset Management.
The Securities and Exchange Commission’s database showed Scion’s registration status as “terminated” as of November 10. Deregistering would imply the fund is not required to file reports with the regulator or any state.
Bets by Scion, which managed $155 million in assets as of March, have long been dissected for hints of looming bubbles and signs of market froth.
In a post on social media platform X on Wednesday, Burry said, “On to much better things Nov 25th.” Scion Asset Management did not immediately respond to a Reuters request for comment.
Burry has stepped up criticism of technology heavyweights, including Nvidia and Palantir Technologies, in recent weeks, questioning the cloud infrastructure boom and accusing major providers of using aggressive accounting to inflate profits from their massive hardware investments.
Bearish AI bets
“Burry’s decision feels less like ‘calling it quits’ and more like stepping away from a game he believes is fundamentally rigged,” said Bruno Schneller, managing director at Erlen Capital Management.
Burry has argued that as companies such as Microsoft, Alphabet-owned Google, Oracle and Meta pour billions into Nvidia chips and servers, they are also quietly stretching out depreciation schedules to make earnings look smoother.
Between 2026 and 2028, those accounting choices could understate depreciation by about $176 billion, inflating reported profits across the sector, he estimated.
“Don’t count him out, just expect him to operate off the grid for a while. He may simply pivot to a family-office setup and run his own capital,” said Schneller.
The investor’s short position against subprime mortgage securities during the housing market crash was chronicled in Michael Lewis’s book, “The Big Short”, and its film adaptation.
His profile on X, titled “Cassandra Unchained,” is seen as a nod to the Greek mythological figure cursed by Apollo to deliver true prophecies that no one would believe.
Investment advisers with assets under management of $100 million or more have to register with the SEC, and are primarily subject to federal regulation instead of state regulation.
The EU has launched an investigation into Google Search over concerns the US tech company has been “demoting” commercial content from news media sites.
The bloc’s executive arm announced the move after monitoring found certain content created with advertisers and sponsors was being given such a low priority by Google that it was effectively no longer visible in search results.
European Commission officials said this potentially unfair “loss of visibility and of revenue” to media owners may be a result of an anti-spam policy Google operates.
Under the rules of the Digital Market Act (DMA), which governs competition in the tech sectors, Google must apply “fair, reasonable and non-discriminatory conditions of access to publishers websites on Google search”.
Commission officials said the investigation was not into the overall indexing of newspapers or their reporting on Google Search, just into commercial content provided by a third parties.
Media partnerships with businesses selling goods or services ranging from holidays to trainers were “normal commercial practice in the offline world” and they should also exist in a fair online marketplace such as Google, officials said.
For example a newspaper may have teamed up with Nike to offer discounts, but there was evidence that under a Google search that sub-domain of the newspaper would be “demoted to a point that users will not be able to find it anymore”, which then impacts the newspapers.
“We are concerned that Google’s policies do not allow news publishers to be treated in a fair, reasonable and non-discriminatory manner in its search results,” said Teresa Ribera, the executive vice-president for clean, just and competitive transition policies at the European Commission.
Officials will ask publishers to submit evidence of any impacts to its traffic and revenues as a result of suspected breaches of fair practices in the coming days, the commission said.
Ribera added: “We will investigate to ensure that news publishers are not losing out on important revenues at a difficult time for the industry, and to ensure Google complies with the Digital Markets Act.
“Today we are taking action to ensure that digital gatekeepers do not unfairly restrict businesses that rely on them from promoting their own products and services.”
skip past newsletter promotion
after newsletter promotion
The EU said it was compelled to take steps to protect traditional media, which was now competing in marketplace online given the recent assertion by the commission president, Ursula von der Leyen, in her state of the union address that the “media at large is at risk” with the arrival of AI and widespread threats to media funding.
Officials stressed the investigation was a “normal non-compliance” inquiry and although fines of up to 20% of revenue could be imposed, that would only be a possibility if Google was found to be practising “systematic non compliance”.
The company said it was not looking at Google advertising services. which were “not part of the organic search”.
LONDON — U.K. economic growth slowed down to a near standstill in the third quarter of the year after a cyberattack halted production at the country’s biggest automaker, official figures showed Thursday.
The slowdown represents a blow to the British government less than two weeks ahead of a crucial budget that is expected to see taxes rise again.
The Office for National Statistics said that the economy grew by 0.1% between July and September from the previous three-month period. That was down on the previous quarter’s 0.3% increase and below market expectations for a 0.2% rise.
The cyberattack on Jaguar Land Rover was a key reason why growth came in lower than expected. The attack, which saw workers sent home on Aug. 31, halted production in the company’s factories as well as suppliers. Operations restarted in October.
The shutdown rippled through the U.K. auto industry. JLR, which is owned by India’s Tata Motors, employs more than 30,000 people, with its supply chain supporting tens of thousands more jobs.
The impact was evident in the growth performance in September, with overall industrial output down 2% during the month and car and trailer manufacturing plunging by 28.6%, its sharpest fall since the height of the coronavirus pandemic in April 2020.
It is the latest set of disappointing economic data for the government after the statistics agency revealed earlier this week that U.K. unemployment has risen to 5%, its highest level for four years.
Statistics point towards a weakening economic backdrop ahead of the budget on Nov. 26, which the government has sought to blame on international factors, such as the uncertainty caused by U.S. tariffs.
Treasury chief Rachel Reeves would have been hoping that stronger economic growth could help bolster tax revenues and support spending plans.
“At my budget later this month, I will take the fair decisions to build a strong economy that helps us to continue to cut waiting lists, cut the national debt and cut the cost of living,” she said.
Reeves has provided clear hints that she is going to have to raise taxes in order to plug a hole in the public finances. She is widely anticipated to increase the basic rate of income tax, something no British government has done for 50 years. It would also break a key manifesto pledge of the Labour government.
It’s a high-stakes time for the government, which is languishing in the opinion polls barely a year-and-a-half after coming to power and Prime Minister Keir Starmer’s favorability ratings deep in negative territory.
Starmer has said that generating economic growth is his government’s central mission. Since the global financial crisis in 2008, the British economy’s growth rates have been lower than the decades before, and that’s had a knock-on impact on the government’s tax take and its ability to fund public services.
“The next challenge will be to ensure that the upcoming budget supports rather than hinders growth — no mean feat given the scale of fiscal consolidation that is expected,” said James Smith, research director at the Resolution Foundation.
Opposition politicians say Labour has done more harm than good since it came to power, and have pinned the blame largely on Reeves’ budget last year, which saw taxes raised on businesses.
MONTRÉAL, Canada — ELYSIS is proud to announce the successful start-up of its 450 kiloampere (kA) designed inert anode cell at the end of an existing potline at the Rio Tinto smelter in Alma, Québec, a defining moment in the transition toward large-scale, low-carbon aluminium production.
This achievement marks the first implementation of inert anode technology at this commercial-size scale. After years of sustained research, development, and rigorous testing, ELYSIS has reached a breakthrough: high-amperage aluminium production with no direct carbon emissions from the smelting process. The ELYSIS® technology also has the potential to improve worker safety, reduce costs, and enhance productivity.
Thanks to the expertise of the ELYSIS team, its partners at Alcoa Corporation and Rio Tinto, and the continued support of the governments of Canada and Québec, ELYSIS has entered a new phase of industrial innovation. Comprehensive and rigorous testing will continue on the large-scale cell, which was designed for industrial demonstration purposes, to gather critical data to support future commercial deployment.
This global first at this commercial size and this amperage reinforces Canada’s position as a leader in sustainable aluminium and reflects ELYSIS’ unwavering commitment to innovation, collaboration, and climate leadership.
Quotes
ELYSIS President and Chief Executive Officer François Perras said: “This historic milestone results from years of relentless innovation and teamwork of all ELYSIS employees and collaborators. While R&D is rarely linear, our combined efforts have turned vision into reality. Today, we’re not just powering a new cell, we’re powering the future of aluminium.”
Rio Tinto Aluminium & Lithium Chief Executive Jérôme Pécresse said: “Today marks a major step for ELYSIS in its journey to commercialize its groundbreaking aluminium smelting technology without direct carbon emissions. Through our involvement in the joint venture, Rio Tinto is reinforcing its commitment to inert anode smelting. The construction of the first demonstration plant using this new technology at our Arvida smelter in Canada underscores its importance as a core pillar of our long-term decarbonization strategy.”
Alcoa Corporation President and Chief Executive Officer William F. (Bill) Oplinger said: “Alcoa founded the aluminium industry and is proud to be part of the development of the next phase of technological advancement. ELYSIS® technology has the potential to fundamentally change the future of our industry, and with the successful implementation at a commercial-size scale, we are one step closer to bringing the technology to market.”
About ELYSIS
ELYSIS is a technology company that emerged from a ground-breaking partnership between two global industry leaders, Alcoa and Rio Tinto. ELYSIS’ goal is to revolutionize the way aluminium is produced worldwide. Our process eliminates all direct greenhouse gases from aluminium smelting, producing oxygen instead. Learn more at www.ELYSIS.com.
Contacts
Please direct all enquiries to media.enquiries@riotinto.com
Double wage rules in China have been clarified under Judicial Interpretation II, reducing ambiguity for employers. The new interpretation explains when double wages apply, clarifies exemptions, and standardizes calculation methods. This article provides practical compliance guidance for HR teams. (Also see our series article: China’s New Judicial Interpretation II on Labor Disputes: Key Themes at a Glance)
On August 1, 2025, China’s Supreme People’s Court (SPC) issued the long-awaited Judicial Interpretation II on the Application of Law in Labor Dispute Cases (Fa Shi [2025] No. 12, hereinafter “Judicial Interpretation II” or Interpretation II”), along with a set of illustrative cases. Both took effect on September 1, 2025.
This interpretation aims to unify judicial standards in labor disputes and clarify several long-standing ambiguities under the PRC Labor Contract Law, including the controversial “double wage” rule for failing to sign written labor contracts.
Find Business Support
Under Article 82 of the Labor Contract Law, employers who do not conclude a written labor contract within one month of employment must pay the employee double wages for each month without a contract. While this rule is designed to protect employees, its application has often been inconsistent, creating compliance risks for foreign-invested enterprises (FIEs). Judicial Interpretation II addresses these gaps by:
Defining when double wage liability applies and when it does not.
Introducing clear exceptions, such as delays caused by force majeure, or the employee’s intentional refusal or gross negligence.
Clarifying calculation standards and the cut-off point for liability once a contract is signed.
For HR teams and compliance managers, understanding these updates is critical to avoid costly disputes and ensure smooth labor relations. This article explains when double wages must be paid, how to calculate them, and what the exemptions mean for employers under the latest judicial guidance.
When must employers pay double wages?
Under Article 82 of the PRC Labor Contract Law, employers who fail to conclude a written labor contract within one month from the employee’s start date must pay the employee double wages for each month without a contract, up to a maximum of 11 months. Similarly, if an employer fails to enter into an open-ended labor contract when legally required, double wages apply from the date such obligation arises.
However, the original law did not specify any exceptions to this rule, which often led to disputes and inconsistent judgments. In practice, circumstances can be complex, placing all liability on the employer may be unfair when delays result from factors beyond their control. Judicial Interpretation II addresses this gap by introducing clear exemptions and calculation standards, reducing uncertainty for both employers and employees.
No double wage liability when the employer is not at fault
Article 7
Where a laborer requests the employer to pay double wages on the grounds that the employer failed to conclude a written labor contract, the people’s court shall support such claim in accordance with the law, except where the employer adduces evidence to prove any of the following circumstances: (1) The failure to conclude a contract was due to force majeure; (2) The failure to conclude a contract was due to the laborer’s own intent or gross negligence; (3) Other circumstances as provided by laws or administrative regulations.
In practice, courts have recognized that not all failures to sign a written labor contract should automatically result in double wage liability. For example, the Shanghai High People’s Court Opinions on Applying the Labor Contract Law state that if an employer has fulfilled its good-faith obligations, and the failure to sign was due to force majeure, unexpected circumstances, or the employee’s refusal, such cases do not constitute “failure to conclude a written labor contract” by the employer.
Building on these regional practices, Judicial Interpretation II (Article 7) now provides nationwide clarity by adopting a more restrictive and fair approach. It specifies that when an employee claims double wages for lack of a written contract, courts will not support the claim if the employer can prove any of the following:
Force majeure caused the failure to sign;
The employee acted with intentional refusal or gross negligence; and
Other circumstances prescribed by law or administrative regulations.
This provision emphasizes substantive review of the reasons behind the failure to sign. If the employer can show evidence that it delivered a written or electronic contract and had no deliberate intent to avoid signing, it may be exempt from double wage liability, even if the contract was ultimately not signed. This demonstrates the importance of documenting contract delivery and communication efforts as part of HR compliance.
Force majeure situations
Force majeure, recognized under civil law as a ground for exemption from liability, also applies in labor contract disputes. If an employer cannot sign a contract due to force majeure, and there is a direct causal link between the event and the failure to sign, the employer bears no fault and is exempt from paying double wages. However, the burden of proof lies with the employer to establish this causal connection.
Employee fault
When the failure to sign is due to the employee’s intentional act or gross negligence, the employer is not required to pay double wages. Judicial practice supports this principle: if the employer has fulfilled its good-faith obligation to conclude the contract, and the responsibility lies entirely with the employee, courts typically reject double wage claims.
Find Business Support
For example, in Illustrative Case No. 3 released alongside Interpretation II, the employer repeatedly urged the employee to renew the contract, but the employee refused, hoping to claim double wages by citing company dissolution rumors. The court ruled that the employee’s intentional refusal absolved the employer of liability. Similarly, for employees in HR or managerial roles responsible for contract administration, failure to sign may often be attributed to their own gross negligence or intent, and courts will allocate responsibility accordingly.
Notably, during the drafting process, the exemption clause evolved from “due to the employee’s own reasons” to “due to the employee’s intentional act or gross negligence,” reflecting a more precise and rigorous standard focused on employee fault.
No double wage when the contract is extended automatically
Article 8
Where the term of a labor contract expires and any of the following circumstances applies, the people’s court shall determine that the term of the labor contract is automatically extended in accordance with the law, and it shall not be deemed as a failure by the employer to conclude a written labor contract: (1) The employer is prohibited from terminating the labor contract as provided in Article 42 of the Labor Contract Law; (2) The service period has not yet expired as provided in Article 17 of the Implementation Regulations of the Labor Contract Law; (3) The term of office has not yet expired as provided in Article 19 of the Trade Union Law.
Judicial Interpretation II (Article 8) confirms that when a labor contract expires but is automatically extended by law, the employer is not liable for double wages during the extension period. This aligns with mainstream judicial practice and addresses situations where employers cannot renew contracts due to statutory restrictions.
Under the Labor Contract Law and related regulations, automatic extension applies in the following cases:
Article 42 of the Labor Contract Law: The employer is prohibited from terminating the contract, such as when the employee is:
Undergoing medical treatment for illness or non-work injury;
Pregnant, on maternity leave, or in breastfeeding period;
In the statutory medical treatment period or work injury recovery period;
Diagnosed or suspected of occupational disease;
Within five years of the statutory retirement age after 15 years of continuous service.
Article 17 of the Implementing Regulations of the Labor Contract Law: The agreed service period has not yet expired.
Article 19 of the Trade Union Law: The employee serves as a full-time chairperson, vice-chairperson, or committee member of a grassroots trade union, and the term has not ended.
In these scenarios, the law deems the contract extended, even if the employer does not sign a new written contract. Because the employee’s rights remain protected, there is no need to impose double wage liability. This rule prevents employers from being penalized for circumstances beyond their control, such as statutory prohibitions or ongoing obligations.
No double wage liability under deeded open-ended contracts
Article 9
Where there is evidence to prove the existence of circumstances as specified in Paragraph 3 of Article 14 of the Labor Contract Law, i.e., “it shall be deemed that the employer has concluded an open-ended labor contract with the laborer,” and the laborer requests to conclude a written labor contract with the employer, the people’s court shall support such claim in accordance with the law; where the laborer requests the employer to pay double wages for the period deemed as an open-ended labor contract on the grounds that the employer failed to timely supplement the written labor contract, the people’s court shall not support such claim.
Judicial Interpretation II (Article 9) narrows the scope of double wage claims in cases involving open-ended labor contracts. Under Article 14(3) of the Labor Contract Law, if an employer fails to sign a written contract for one year from the employee’s start date, the law deems that an open-ended labor contract has been established. In such cases, the employee may request the employer to supplement the written contract, but cannot claim double wages for the deemed period.
This clarification reinforces the punitive nature of double wage liability. It is intended to encourage timely contract signing, not to create windfall gains for employees. By limiting claims, the rule prevents abuse of rights and strikes a balance between protecting employees and avoiding excessive penalties for employers.
How to calculate double wages
Find Business Support
Judicial Interpretation II (Article 6) provides a clear calculation method for double wages, resolving inconsistencies in past practice. The rule clarifies that if an employer fails to conclude a written labor contract in accordance with the law, double wages shall be calculated on a monthly basis; if the period is less than one month, calculation shall be based on the actual working days of that month.
This change standardizes the approach for partial months, ensuring precision and fairness. For example, if an employee works 20 days without a written contract and their monthly salary is RMB 5,000, the double wage should be calculated based on the actual working days, not an estimated or “blurred” formula.
Article 6
Where an employer fails to conclude a written labor contract with a laborer in accordance with the law, it shall pay the laborer double wages on a monthly basis; if the period is less than one month, payment shall be calculated based on the actual working days in that month.
“Payable days” vs “actual working days”
The final text of Interpretation II replaces the draft term payable days (“计薪日”) with actual working days (“实际工作日”) as the basis for calculation. This distinction matters because:
Payable days include statutory holidays as paid days.
Actual working days exclude statutory holidays and count only days when the employee actually worked.
For example, in October 2025 (31 days), with nine weekend rest days (including adjusted rest days) and four statutory holidays (three days National Day holiday + 1 day Mid-Autumn Festival):
Payable days = 31 days – 9 weekends = 22 days.
Actual working days = 31 days – 9 weekends – 4 holidays = 18 days
Of course, the above discussion is based on normal circumstances. In special cases, such as when an employee works on rest days or statutory holidays, those days are naturally counted as actual working days as well.
20.67 days vs. 21.75 days
One common misunderstanding is confusing the “payable days” and “actual working days” mentioned in Judicial Interpretation II with the monthly averages defined in the Ministry of Human Resources and Social Security (MOHRSS) notice on wage conversion standards (MOHRSS Notice [2025] No. 2). The MOHRSS document specifies:
Average monthly working days: (365 days − 104 weekends − 13 holidays) ÷ 12 = 20.67 days/month
Average monthly payable days: (365 days − 104 weekends) ÷ 12 = 21.75 days/month
These figures are annual averages used for standardizing wage calculations (for example, converting a monthly salary to a daily or hourly rate). They smooth out variations in month length and holiday distribution. By contrast, Judicial Interpretation II refers to the actual number of working days in a specific month, not an annual average. This distinction is critical for calculating double wages accurately.
Natural month or rolling month?
Judicial Interpretation II states that double wages for a full month should be calculated by month. But what does “month” mean in this context?
In judicial practice, “by month” is generally understood as a natural month (calendar month, from the first day to the last day of the same month. This interpretation ensures clarity and operational consistency. If “month” were treated as any arbitrary 30 or 31-day period, calculation start and end points would become confusing and prone to disputes.
Based on our understanding, Article 6 of Judicial Interpretation II supports this reading:
Full month: A complete natural month (for example, all of June), calculated based on the monthly salary.
Partial month: Any incomplete natural month, such as the month of entry (not starting on the first day) or the month of departure (not ending on the last day), calculated based on actual working days.
Example: How to calculate double wages
Suppose an employee joins on July 15, 2025, with a monthly salary of RMB 20,000, and the company fails to sign a written labor contract. The employee works full attendance from August 15 to August 31 (11 actual working days), works normally throughout September, and then resigns on October 10 after working six days and taking four statutory holidays (National Day and Mid-Autumn). Normal wages (including overtime payment) have already been paid, but the employee claims double wages for the period without a contract (August 15–October 10).
For employers, preventing double wage disputes starts with proactive compliance and thorough documentation. First and foremost, companies should establish a standardized contract management process to ensure written labor contracts are signed within the statutory one-month period.
When delays occur due to circumstances beyond the employer’s control, such as force majeure or the employee’s refusal to sign, it is critical to retain evidence. This includes official emergency notices, disaster alerts, and written or electronic communication records (emails, SMS, chat logs) showing repeated attempts to conclude the contract. Such documentation demonstrates good-faith efforts and can exempt the employer from liability under Judicial Interpretation II.
Employers should also be aware of automatic extension scenarios. Before a labor contract expires, HR teams must verify whether a statutory extension applies, such as during maternity leave, medical treatment, or union duties. In these cases, issuing a written extension notice that specifies the extended term helps prevent misunderstandings and disputes.
Finally, HR professionals should be trained on the correct calculation rules for double wages. Calculations should always be based on the actual working days in the specific month. By combining timely contract execution, clear communication, and meticulous record-keeping, employers can significantly reduce compliance risks and protect their interests.
About Us
China Briefing is one of five regional Asia Briefing publications. It is supported by Dezan Shira & Associates, a pan-Asia, multi-disciplinary professional services firm that assists foreign investors throughout Asia, including through offices in Beijing, Tianjin, Dalian, Qingdao, Shanghai, Hangzhou, Ningbo, Suzhou, Guangzhou, Haikou, Zhongshan, Shenzhen, and Hong Kong in China. Dezan Shira & Associates also maintains offices or has alliance partners assisting foreign investors in Vietnam, Indonesia, Singapore, India, Malaysia, Mongolia, Dubai (UAE),Japan, South Korea, Nepal, The Philippines, Sri Lanka, Thailand, Italy, Germany, Bangladesh, Australia, United States, and United Kingdom and Ireland.
For a complimentary subscription to China Briefing’s content products, please click here. For support with establishing a business in China or for assistance in analyzing and entering markets, please contact the firm at china@dezshira.com or visit our website at www.dezshira.com.
This tripartite agreement will empower public and private enterprises with locally hosted solutions that comply with regional data protection laws and enable digital independence.
PRESS RELEASE
NAIROBI, KENYA | MUMBAI, INDIA, November 13, 2025: In a landmark move to advance Africa’s digital transformation agenda, Tata Consultancy Services (TCS) (BSE: 532540, NSE: TCS), Sybyl, and IXAfrica Data Centre Limited (iXAfrica) have announced a strategic partnership to establish and scale sovereign cloud infrastructure in Kenya and other East African countries. Through a Memorandum of Understanding with both Sybyl and iXAfrica, TCS aims to empower governments, enterprises, and innovators with secure, locally hosted cloud offerings that comply with national data residency and sovereignty requirements, marking a major milestone in Africa’s journey towards digital independence.
TCS, Sybyl and iXAfrica will combine their strengths to build a robust foundation for digital transformation in East Africa. TCS will bring its sovereign cloud and global cloud expertise, Sybyl will bring its regional engineering and customer support expertise, and iXAfrica will provide secure, scalable AI ready data centre infrastructure. With complementary strength, the trio will ensure enterprises benefit from world-class technology, local implementation, and resilient data hosting. As Africa doubles down on its digital transformation agenda, data sovereignty has become a defining issue across the continent. Several national governments and enterprises are increasingly seeking solutions that ensure data is housed within a country’s borders, regulated as per regional laws, and managed through secure and robust infrastructure. This partnership directly addresses that urgent need by offering a trusted, built-in-Africa cloud environment.
TCS will deploy TCS Sovereign Secure CloudTM, a bespoke offering for government, public enterprises, and regulated industries, that offers a sovereign cloud with integrated AI to drive data, operational, and digital sovereignty. It will provide the sovereign cloud architecture, deployment frameworks, and security expertise, drawing from its global leadership in IT services, consulting, and digital transformation.
Satishchandra Doreswamy, Vice President & Head, Cloud Unit – Growth Markets, TCS,“We offer a resilient and future-ready cloud infrastructure, powered by AI-driven intelligence, that can be tailored to specific needs of our customers. With built-in compliance to global and local regulatory authorities, our sovereign cloud fuels future-forward business models while meeting the most stringent standards for privacy and regulatory requirements. It is the ideal solution for countries and enterprises that are looking to safeguard their digital sovereignty through robust cloud technology.”
Sybyl, one of East Africa’s leading systems integrators, will lead local implementation, support, and customer enablement, leveraging its deep regional expertise in enterprise technology solutions and managed services. Shailendra Yadav, CEO, Sybyl Kenya & Tanzania, said, “Digital independence must deliver real gains. By running sovereign cloud in iXAfrica’s AI-ready campus along with TCS’ cloud expertise, we cut currency exposure, foreign policy risks, keep services reachable on local routes during outages, and create skilled jobs for Kenyans and Africans as a whole”
Home to East Africa’s leading carrier-neutral and AI-ready data centre campus (NBOX1), iXAfrica will provide the secure, scalable, and energy-efficient infrastructure hosting the Sovereign Cloud. Snehar Shah, CEO, iXAfrica, said, “Data sovereignty is the cornerstone of Africa’s digital future. By hosting Sovereign Cloud infrastructure within iXAfrica’s AI-ready campus, we are ensuring that African data stays in Africa, secure, sustainable, and ready to power the next generation of innovation.”
A sovereign cloud infrastructure leverages economies of scale of cloud computing while strictly protecting data, complying with privacy needs, ensuring operational sovereignty, and enabling easy access to the full range of cloud services with powerful computing. It has applications across sectors such as banking, telecom, public sector, and enterprise sectors. By leveraging locally hosted and globally secure cloud environments, both public and private enterprises are empowered to operate within a framework that fully supports compliance with national data protection laws. This ensures that sensitive data remains within the country’s borders while adhering to rigorous regional and international security standards.
TCS’ sovereign cloud offering is designed to future-proof companies by providing access to advanced AI and analytics capabilities. Enterprises will also gain the advantage of end-to-end managed services and local technical expertise. This comprehensive support enables organisations to seamlessly adopt, operate, and scale their cloud solutions, fostering confidence and resilience in the rapidly evolving digital landscape.
This initiative is aimed at creating jobs that will employ local talent, strengthen local digital infrastructure, and position East Africa as a strategic technology hub for Africa as a whole. TCS has operated in Africa for almost two decades and has over 50 clients in the region. It serves most of the region’s large enterprises including top telecommunication companies, leading banking and insurance firms, as well as utilities and public enterprises. Additionally, TCS has been awarded the Top Employer Award for nine consecutive years in the region.