Prostate cancer affects one in five Australian men, making it the most common cancer in the country. Now, researchers at the Garvan Institute of Medical Research have produced the world’s most detailed cellular ‘atlas’ of…
Category: 6. Health
-
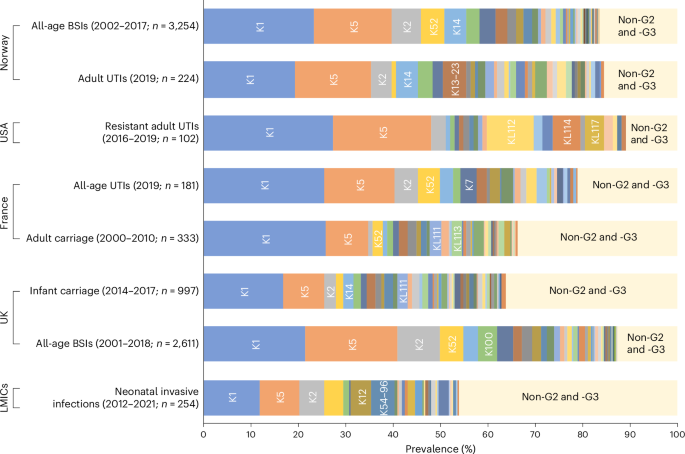
Identification of transporter-dependent capsular loci associated with the invasive potential of Escherichia coli
Mba, I. E. et al. Vaccine development for bacterial pathogens: advances, challenges and prospects. Trop. Med. Int. Health 28, 275–299 (2023).
Google Scholar
Murray, C….
Continue Reading
-

A Common ADHD Med Might Not Raise Psychosis Risk After All
No drug comes without its side effects. A study out today, however, should comfort anyone worried about the long-term consequences of taking methylphenidate, the active ingredient in brand-name drugs like Ritalin, for their…
Continue Reading
-
Placental abruption linked to higher heart risk in children
The risk of developing early cardiovascular disease or dying from cardiovascular disease by the age of 28 was about 4.6 times higher among people born to mothers who had a placental abruption during their pregnancy. This finding…
Continue Reading
-

Anthrax-causing bacteria have dwelled in soil for centuries – cycling through people, animals and earth
The bacteria that cause deadly anthrax disease persist in the earth, a place their ancestors preferred over petri dishes and blood-filled tissues.
The bacteria that cause anthrax are called Bacillus anthracis. In the soil, they hang out and…
Continue Reading
-
Study finds no link between workplace radio wave exposure, brain cancer-Xinhua
MELBOURNE, March 25 (Xinhua) — A new study has found no evidence that occupational exposure to radiofrequency (RF) electromagnetic energy (EME) increases the risk of brain cancer.
The research, led by Australian and European researchers,…
Continue Reading
-
New skin atlas maps over one million cells across the human body
Mount Sinai researchers have published the first organ-wide human skin spatial atlas from across the body. It provides an unprecedentedly detailed view of healthy human skin, revealing cellular composition and functional mechanisms…
Continue Reading
-

Prenatal nutrient gaps show 90% of pregnant US women are deficient in choline
Pregnant women are experiencing deficiencies in crucial prenatal nutrients, including choline, folate, and the omega-3 fatty acids docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA). In the US, 90% of women are deficient in choline, a…
Continue Reading
-

NHS hospital waited two days before raising alarm about meningitis outbreak – BBC
- NHS hospital waited two days before raising alarm about meningitis outbreak BBC
- Cases of invasive meningococcal disease notified in Kent GOV.UK
- Rapid reaction: What is meningitis B? The London School of Hygiene & Tropical Medicine
- Judicial Storm:…
Continue Reading
-

Review of the European Association for Haemophilia and Allied Disorders (EAHAD) 19th Annual Congress
IN the vibrant city of Dublin, Ireland, over 2,000 delegates from over 77 countries gathered for the 19th annual European Association for Haemophilia and Allied Disorders (EAHAD) Congress, to recognise the history, advancements, and persisting…
Continue Reading