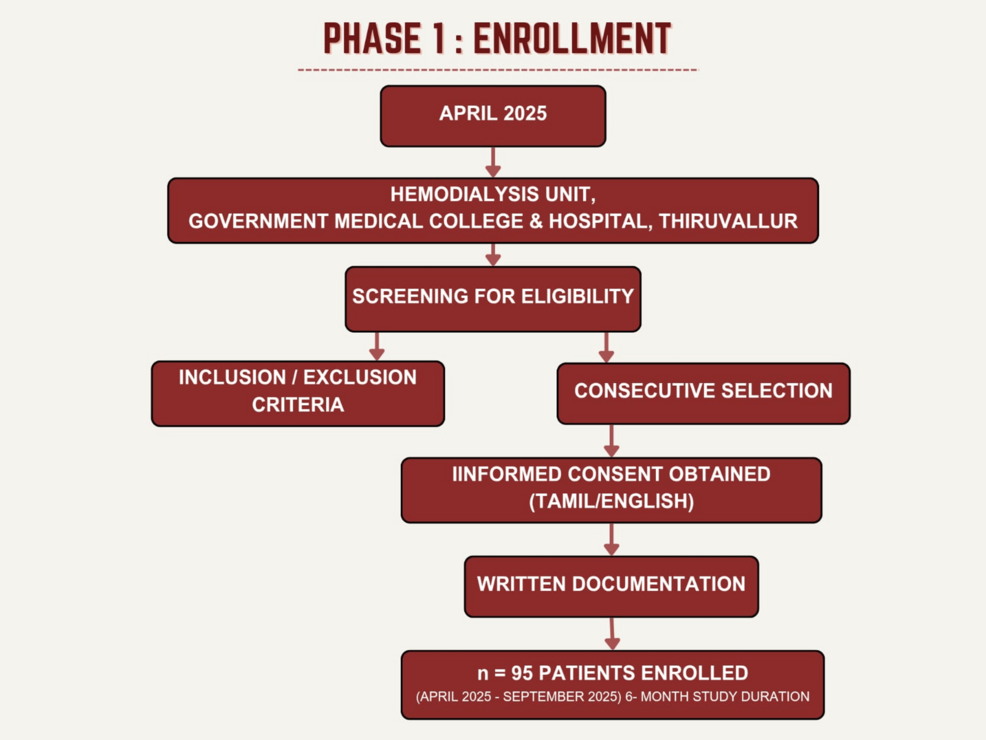
NEW long-term evidence demonstrates that cognitive training focused on processing speed can significantly reduce the risk of a dementia diagnosis decades later, offering one of the strongest indications yet that targeted brain training could…
Category: 6. Health
-
Colorectal cancer is increasing among young people, as James Van Der Beek’s death reminds us – cancer experts explain ways to decrease your risk
An increasing number of people are dying of colorectal cancer at a young age, including those as young as 20. Actor James Van Der Beek, who was diagnosed with colorectal cancer in 2023, died at age 48 on Feb. 11, 2026, bringing the disease back…
Continue Reading
-

Al-Sayeh reveals a new toll of pulmonary tuberculosis infections and warns of the worsening epidemiological situation inside migrant shelter centers
Tripoli – The Director of the National Center for Disease Control, Haider Al-Sayeh, announced a new tally of pulmonary tuberculosis cases in the country. He warned of a worsening epidemiological situation within irregular migrant…
Continue Reading
-

Could Lower Protein Intake Help Prevent Liver Cancer? New Research Points to a Possible Link
A recent study suggests reducing dietary protein may slow liver cancer development in people with impaired liver function, but healthy individuals likely do not need to worry.
New research indicates that lowering protein intake could…
Continue Reading
-

Measles vaccine plea issued ahead of half term – BBC
- Measles vaccine plea issued ahead of half term BBC
- West Midlands measles vaccine plea ahead of half term BBC
- Families encouraged to check MMR vaccinations ahead of half term Black Country Radio
- Freshers urged to get MMR jab amid measles…
Continue Reading
-
Sylvester Cancer Center Identifies Molecular Mechanisms Behind Chemotherapy Resistance and Explores Survivorship Strategies – geneonline.com
- Sylvester Cancer Center Identifies Molecular Mechanisms Behind Chemotherapy Resistance and Explores Survivorship Strategies geneonline.com
- Carolina Paula Bañuelos: Insights from DNA Damage Biology with Clinical Implications Oncodaily
Continue Reading
-

Cambodia records first human case of bird flu in 2026
In this file photo dated Feb 12, 2024, farm geese walk across a road outside Phnom Penh, Cambodia. (PHOTO/AP) PHNOM PENH – A 30-year-old man from southwest Cambodia’s Kampot province had been confirmed positive for H5N1 human avian influenza,…
Continue Reading
-
Molecular evolution and diversity of the norovirus RNA-dependent RNA polymerase
Lucero, Y., Matson, D. O., Ashkenazi, S. & George, S. O’Ryan, M. Norovirus: facts and reflections from Past, Present, and future. Viruses 13, 2399. https://doi.org/10.3390/v13122399 (2021).
Continue Reading