- ‘Nobody can afford to have meningitis’, mum says BBC
- Cases of invasive meningococcal disease notified in Kent GOV.UK
- Meningitis outbreak: what you need to know GOV.UK blogs
- Judicial Storm: Tuju Case Exposes Fragility of Kenyan Courts
Category: 6. Health
-
'Nobody can afford to have meningitis', mum says – BBC
-
Systematic review identifies stress-induced biological triggers in oncology
Stress is a constant companion in the oncologist’s office. It appears at the time of diagnosis, increases with each stage of treatment, and often does not resolve even after therapy formally ends. It accompanies therapeutic…
Continue Reading
-
Most Americans don’t know this food raises colon cancer risk
March is National Colorectal Cancer Awareness Month, and a new poll from the Physicians Committee for Responsible Medicine and Morning Consult highlights a major knowledge gap. Nearly half of Americans do not realize that eating processed meat is…
Continue Reading
-
Microscopic sensors could revolutionize diagnosis and monitoring of cancer
Microscopic sensors that are as thin as a strand of hair but capable of taking multiple measurements simultaneously could revolutionize the diagnosis and monitoring of diseases like cancer.
Researchers from…
Continue Reading
-

More than 1 million illegal health products including cough syrup, sex drugs seized in Singapore in 2025
March 25, 2026
SINGAPORE – More than 1.06 million units of illegal health products worth over $750,000 were seized in 2025, an increase of around 10 per cent from the previous year, said the Health Sciences Authority (HSA) on March 24.
Most of…
Continue Reading
-
Brain scans suggest nature exposure may boost mood and cut negative feelings – Medical Xpress
- Brain scans suggest nature exposure may boost mood and cut negative feelings Medical Xpress
- Walking is good for your mental health The Baylor Lariat
- 3 real biological benefits to going outside (and the actual science behind why it makes us feel…
Continue Reading
-

Kimchi bacteria flush nanoplastics from gut with added heart health benefits
The World Institute of Kimchi study has found that a lactic acid bacterium from kimchi can help remove nanoplastics from the body by binding them in the intestine. Meanwhile, another new study using South Korean health data has found that higher…
Continue Reading
-

Wholegrain rye changes gut bacteria and lowers inflammation in obesity trial
A 12-week randomized trial found that wholegrain rye did not beat refined wheat for weight loss, but it did reduce inflammation and shift gut microbiota and short-chain fatty acids in potentially beneficial ways.
Key takeaways
Rye…
Continue Reading
-

Navigating New Horizons in Neuroendocrine Prostate Cancer
In a conversation with CancerNetwork® following the
19th Annual New York GU Cancers Congress® , Rahul Aggarwal, MD, touched upon on the shifting paradigm of neuroendocrine prostate cancer (NEPC) based on a presentation he gave at the…Continue Reading
-
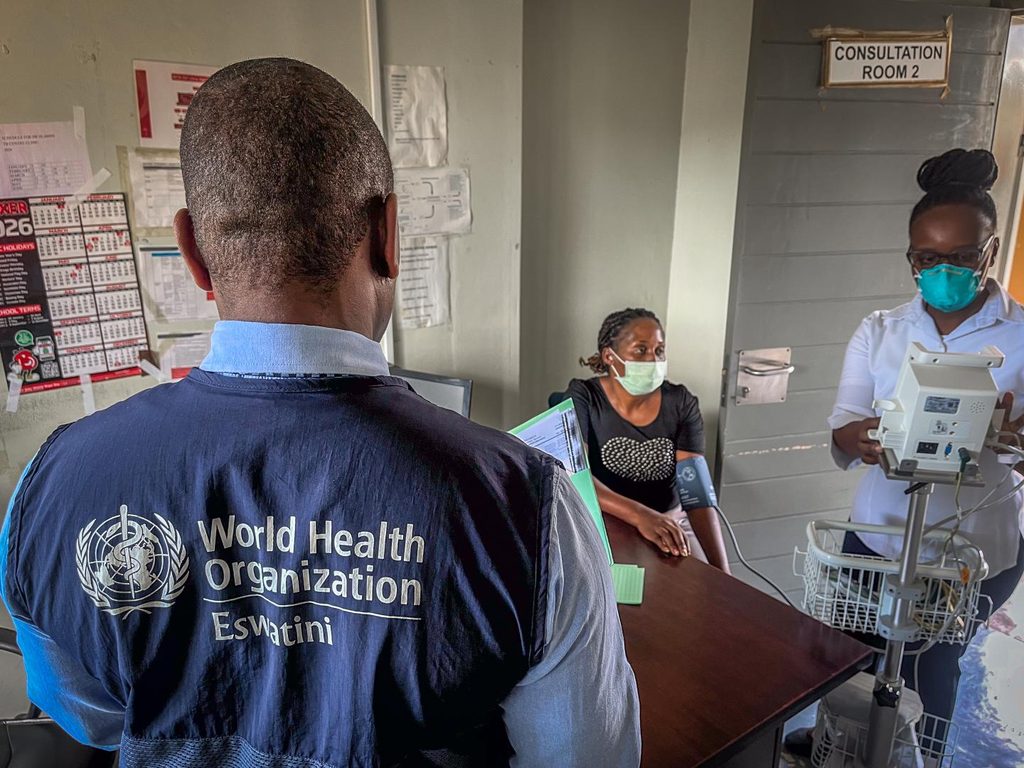
Treatment of multidrug-resistant tuberculosis in Eswatini shows encouraging results | Africa News
Geneva, Switzerland, 24 March 2026- /African Media Agency (AMA)/- “There are various reasons for medication failure,” says Majaha Mtshali, tuberculosis (TB) focal person and staff nurse at Piggs Peak hospital in northwestern Eswatini. “When…
Continue Reading