The Medicines and Healthcare products Regulatory Agency (MHRA) has today, 11 February 2026, announced changes to the use of the Chikungunya vaccine, IXCHIQ, following recommendations by the Commission on Human Medicines (CHM), the government’s…
Category: 6. Health
-
Uganda confirms Crimean-Congo haemorrhagic fever case in central region-Xinhua
KAMPALA, Feb. 11 (Xinhua) — Uganda’s Ministry of Health on Wednesday confirmed a case of Crimean-Congo haemorrhagic fever (CCHF) in Kyankwanzi District in central Uganda.
In a statement issued here, the ministry said laboratory tests on…
Continue Reading
-

A Rare Skin Cancer Diagnosis Requires a Balancing Act Between Suppressing and Boosting the Immune System
As a kidney transplant recipient, Paris Malachias was accustomed to dealing with skin cancer. It’s a common side effect of post-transplant immunosuppressants, which leave transplant recipients extra sensitive to sun, and…
Continue Reading
-
South Asian adults in the U.S. have higher prevalence of risk factors for heart disease
South Asian adults in the U.S. report doing many of the right things for heart health, yet they show significantly higher rates of prediabetes, diabetes and hypertension than white and Chinese adults, and higher than or roughly…
Continue Reading
-

NeuroVoices: Katrina Bawden, MSN, MSCN, FNP-C, on Emerging Therapies and Women’s Health Priorities in Multiple Sclerosis | NeurologyLive
Care for patients living with
multiple sclerosis (MS) has continued to change in recent years, alongside developments in disease-modifying therapies, evolving because of considerations related to women’s health, and increased attention to…Continue Reading
-
CAR T Therapy Shows Promise for Alzheimer’s Treatment
Chimeric antigen receptor (CAR) T cell therapy, a type of immunotherapy that leverages the immune system to combat diseases, is a powerful treatment option for certain cancers. The treatment relies on genetically modified T cells — a type…
Continue Reading
-

Robotic Secondary Cytoreductive Surgery Outcome
ROBOTIC secondary cytoreductive surgery enabled rapid complete removal of three extrapelvic ovarian cancer recurrences in one case.
Robotic Secondary Cytoreductive Surgery Across Three Sites
Secondary cytoreductive surgery (SCS) is…
Continue Reading
-
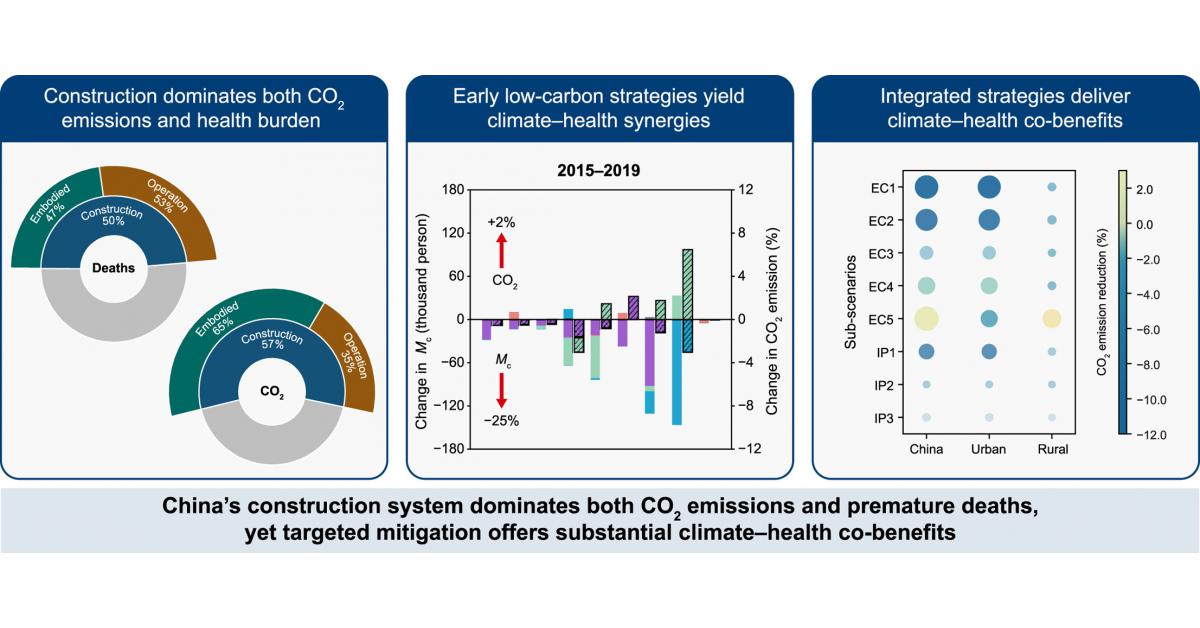
China’s building boom emerges as a hidden driver of air-pollution deaths
Construction as a major driver of CO2 emissions and air-pollution health burdens in China.
GA, UNITED STATES, February 11, 2026 /EINPresswire.com/ — Construction-related activities are responsible for roughly half of China’s premature…
Continue Reading
-

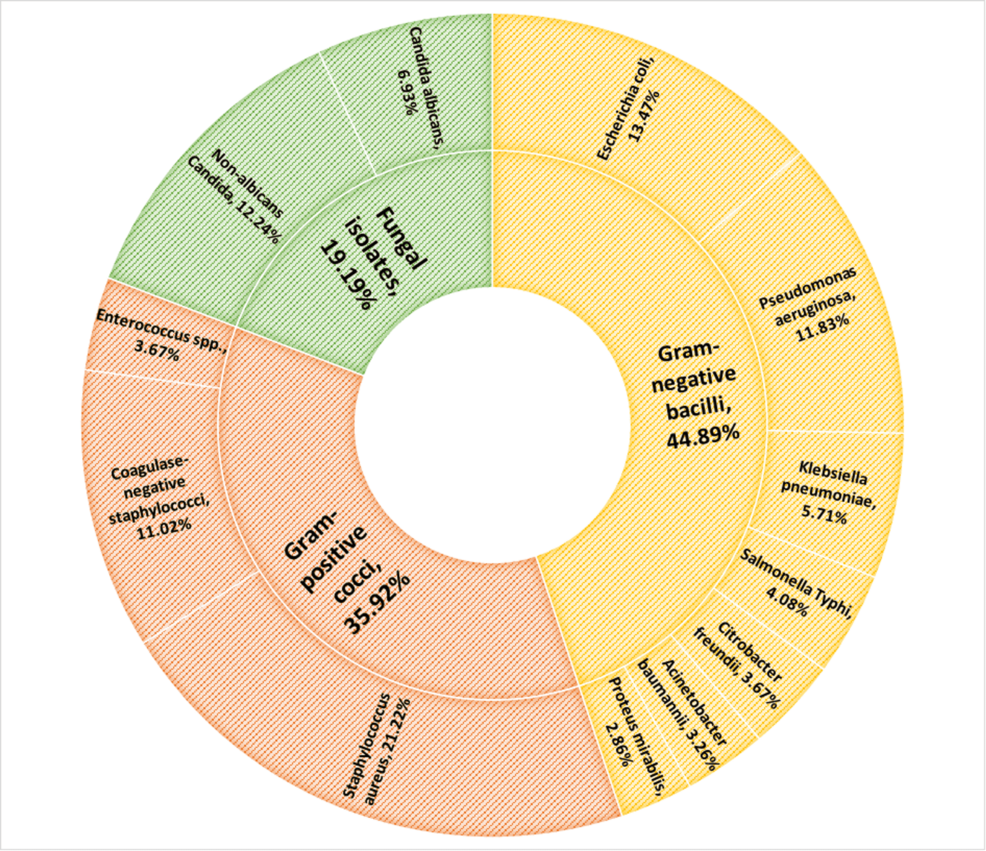
How Missed HAI Targets Reveal Need for Enhanced Infection Control
A report revealed a need for improved and efficient infection control and prevention systems in healthcare facilities. In 2024, Oregon recorded 1,000 hospital-acquired…
Continue Reading