In a recent study, investigators compared treatment protocols for oligometastatic prostate cancer, analyzing metastasis-directed therapy (MDT) plus the standard of care (SOC) versus SOC alone to discern the overall effectiveness of MDT for this…
Category: 6. Health
-

Obesity Linked to One in Ten Global Infectious Disease Deaths, Large Study Finds
A new large-scale study published in The Lancet has found that obesity dramatically increases the risk of hospitalization and death from a wide range of infectious diseases, adding to growing evidence that excess body weight plays a critical…
Continue Reading
-
Alcohol Addiction Alters Endocannabinoid Genes in the Brain
Chronic alcohol consumption profoundly alters gene expression in key brain regions involved in reward, impulse control, and decision-making, according to a study led by researchers at the Institute for Neurosciences, a joint center of Miguel…
Continue Reading
-

Experts urge for more research into youth-onset diabetes
Obesity, gut bacteria, and metabolic conditions in childhood and adolescence need additional investigation to protect children at risk of youth-onset diabetes, according to researchers from the University of Toronto.1
The research team…
Continue Reading
-
MHC class II marks stronger immune response and longer survival in ovarian cancer
A new study sheds light on why some patients with the most aggressive form of ovarian cancer respond better to treatment than others. Tumors positive for a molecule called MHC class II are linked to stronger immune responses and…
Continue Reading
-
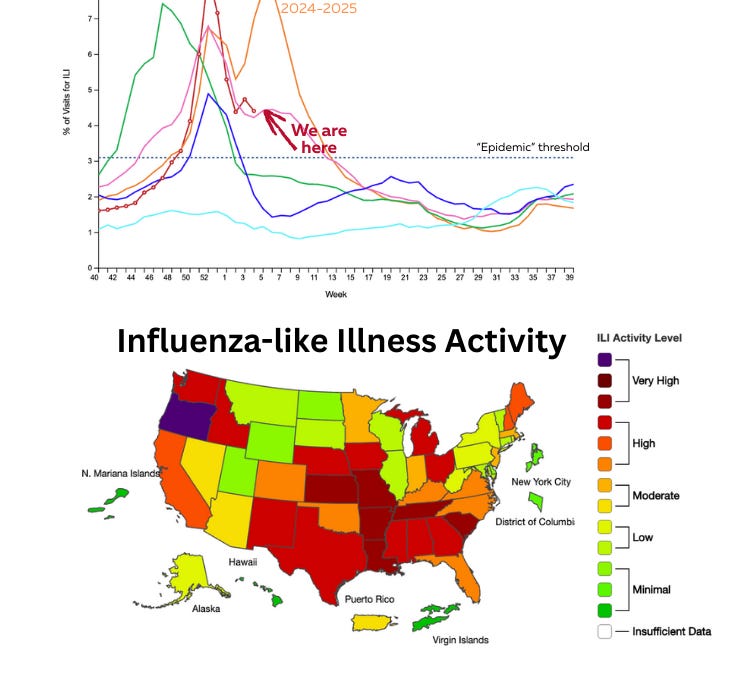
TrumpRx, Super Bowl commercials, flu B is here, and more
I hope you had a great weekend! I’m still buzzing from the rare combination of the Olympics and the Super Bowl halftime show. Both are powerful reminders of community, connection, and love. Moments like that make me feel deeply proud of this…
Continue Reading
-

Anterior crossbite linked to increased tooth loss risk
Crooked teeth or a misaligned bite can cause a whole host of problems, including speech issues and/or difficulty eating or properly cleaning teeth. What many don’t consider, however, is how a bad bite or crowded teeth can affect the…
Continue Reading
-

Brazilian study shows increase in Covid-19-era substance abuse-related deaths
The societal and economic impacts of the Covid-19 pandemic included a variety of downstream effects on health endpoints worldwide. Among them, one widely recorded phenomenon was the increase in substance…
Continue Reading