Peer-reviewed research in Antiviral Research reveals the clinical impact of treatments and immune-supportive protocols.
WASHINGTON, Feb. 11, 2026 /PRNewswire/ — As measles…
Peer-reviewed research in Antiviral Research reveals the clinical impact of treatments and immune-supportive protocols.
WASHINGTON, Feb. 11, 2026 /PRNewswire/ — As measles…
A novel CAR-T cell approach targets amyloid plaques in preclinical Alzheimer models, raising the possibility that engineered immune therapies could reshape future treatment strategies while major clinical questions remain.
Study:

New from the

Data from a recent study showed that an osteo strength-based exercise program was safe and feasible in promoting improved bone health among women with breast cancer receiving endocrine therapy.
Lu Chen, PhD, RN, of the Beijing Tsinghua Changgung…
You don’t have permission to access “http://www.mountsinai.org/about/newsroom/2026/major-depressive-disorder-shares-immune-abnormalities-and-potential-therapeutic-targets-with-inflammatory-skin-diseases-according-to-new-study”…
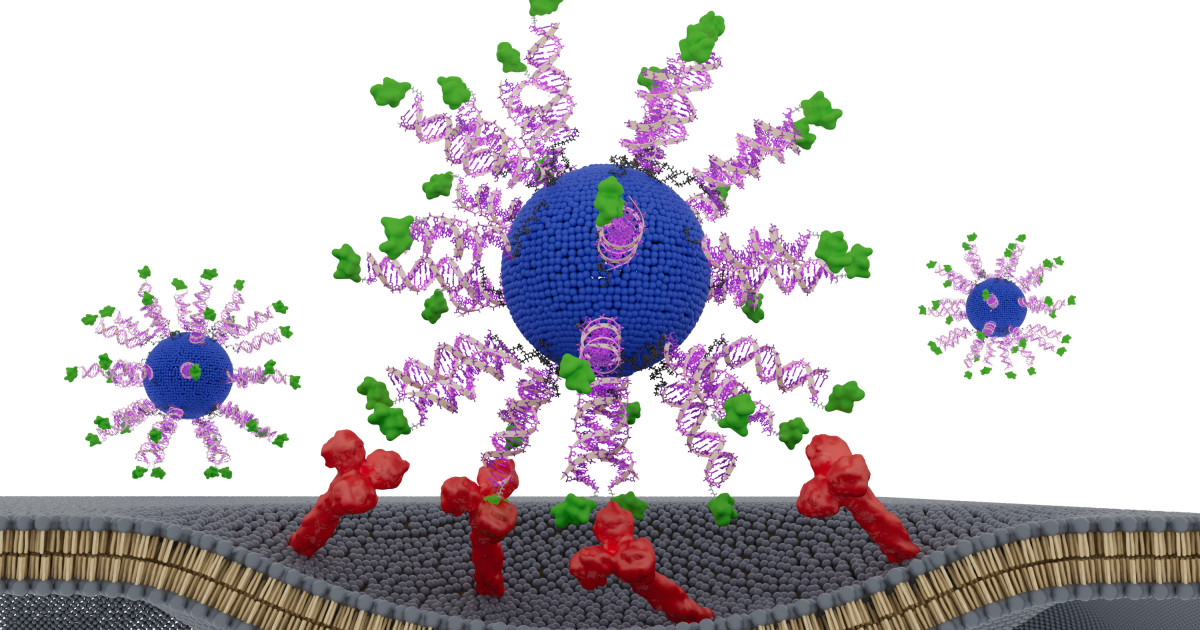
Throughout the past decade, Northwestern University scientists have uncovered a striking principle of vaccine design: Performance depends not only on vaccine components but also on vaccine structure.
After proving this…

STAT The NCI director didn’t cite new evidence that prompted the agency to look into it. The National Cancer Institute, the federal research agency charged with leading the war against the…


Azurity Pharmaceuticals has announced that lisdexamfetamine dimesylate (Arynta) oral solution will be available mid-2026 for treating attention-deficit/hyperactivity disorder (ADHD) in adults and pediatric patients aged 6 years and older.1…

The Medicines and Healthcare products Regulatory Agency (MHRA) has today, 11 February 2026, announced changes to the use of the Chikungunya vaccine, IXCHIQ, following recommendations by the Commission on Human Medicines (CHM), the government’s…