In a conversation with CancerNetwork® following the
Category: 6. Health
-

Navigating New Horizons in Neuroendocrine Prostate Cancer
19th Annual New York GU Cancers Congress® , Rahul Aggarwal, MD, touched upon on the shifting paradigm of neuroendocrine prostate cancer (NEPC) based on a presentation he gave at the… -
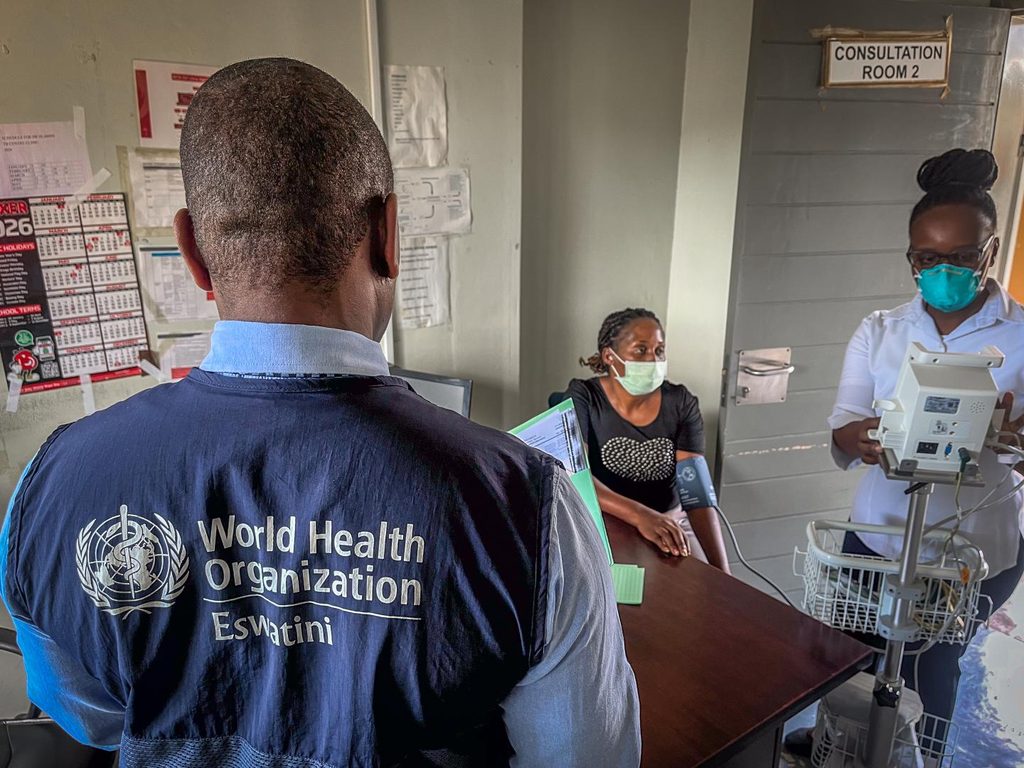
Treatment of multidrug-resistant tuberculosis in Eswatini shows encouraging results | Africa News
Geneva, Switzerland, 24 March 2026- /African Media Agency (AMA)/- “There are various reasons for medication failure,” says Majaha Mtshali, tuberculosis (TB) focal person and staff nurse at Piggs Peak hospital in northwestern Eswatini. “When…
Continue Reading
-

NASA X-Ray Mission Probes Ancient Supernova
NASA’s IXPE observed the outer rim of the supernova remnant highlighted in purple in the inset. Data from IXPE is combined with data from NASA’s Chandra X-ray Observatory and ESA’s XMM-Newton. The yellow represents low-energy X-rays,…
Continue Reading
-
Is Premature Menopause Associated With Increased CHD Risk?
Premature menopause was associated with an increased lifetime risk of coronary heart disease (CHD) in Black women and White women in the U.S., according to a population-based cohort study published March 18 in JAMA. These findings emphasize the…
Continue Reading
-

What Role Does Amyloid Beta Play in Alzheimer’s?
Original story from the University of California Riverside (CA, USA).
New research suggests Alzheimer’s arises not simply from plaques forming in the brain, but from one protein interfering with the normal job of another.
For…
Continue Reading
-

Continuous wearable monitoring improves postoperative oxygen levels and patient safety
Patients continuously monitored after surgery experienced significantly less time with dangerously low oxygen levels compared to those monitored using routine spot checks, a new study from Wake Forest University School of…
Continue Reading
-

Cerebrospinal fluid marker enhances accuracy in diagnosis of Parkinson’s and Lewy body dementia
An international consortium has achieved a major breakthrough in the diagnosis of neurological diseases. In a recent publication in the scientific journal Nature Medicine, they describe the discovery of a new quantitative biomarker…
Continue Reading
-
South Africa urges collective action to end TB-Xinhua
CAPE TOWN, March 24 (Xinhua) — South African Deputy President Paul Mashatile on Tuesday called for collective action to end tuberculosis (TB), emphasizing that every individual has a role to play as the country marks World TB Day.
…
Continue Reading
-
Study finds new biomarker for cognitive symptoms of schizophrenia, could serve as drug target
The study pinpointed a specific schizophrenia biomarker using which the scientists can identify a subgroup of people who would most likely respond well to this SEAD1-based peptide drug, they said |Image used for…
Continue Reading
-
Medicare reforms improve medication adherence among older adults with heart disease
Medicare beneficiaries with heart disease or major cardiovascular risk factors reported less cost-related medication non-adherence-skipping or reducing doses, delaying prescription fills or foregoing medications due to cost-after…
Continue Reading