- Blanket BP Target Disserves Older Adults Medscape
- The root causes of high blood pressure WFLA
- New Era of Hypertension Care: Protecting Hearts, Preserving Minds: Dr Sushil statetimes.in
- New in Clinical Guidance | High Blood Pressure Focus of New…
Category: 6. Health
-
Blanket BP Target Disserves Older Adults – Medscape
-
Diet Soda and Liver Risk; Pig-to-Human Liver Transplant; Golimumab Approval Expanded – MedPage Today
- Diet Soda and Liver Risk; Pig-to-Human Liver Transplant; Golimumab Approval Expanded MedPage Today
- Diet and sugary drinks raise risk of common liver disease by up to 60%, study finds CNN
- Sugar-sweetened beverages: The health impact of soda,…
Continue Reading
-
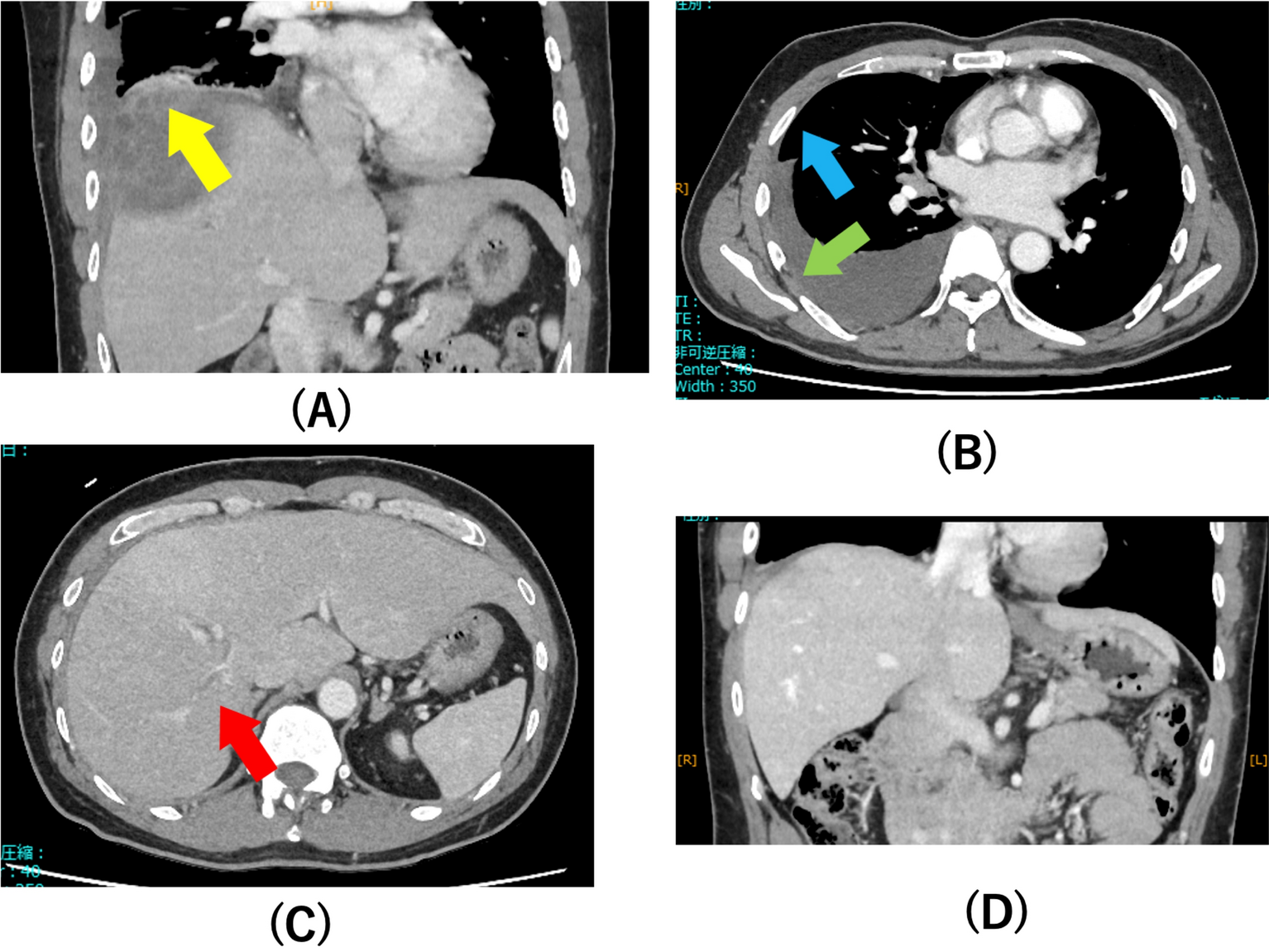
Intrathoracic rupture of amebic liver abscess: a case report and literature review | Tropical Medicine and Health
A 40-year-old bisexual Japanese man presented to our emergency department with pain in the right shoulder and right upper quadrant of the abdomen. Two weeks before presentation, he experienced severe right shoulder pain and consulted a local…
Continue Reading
-
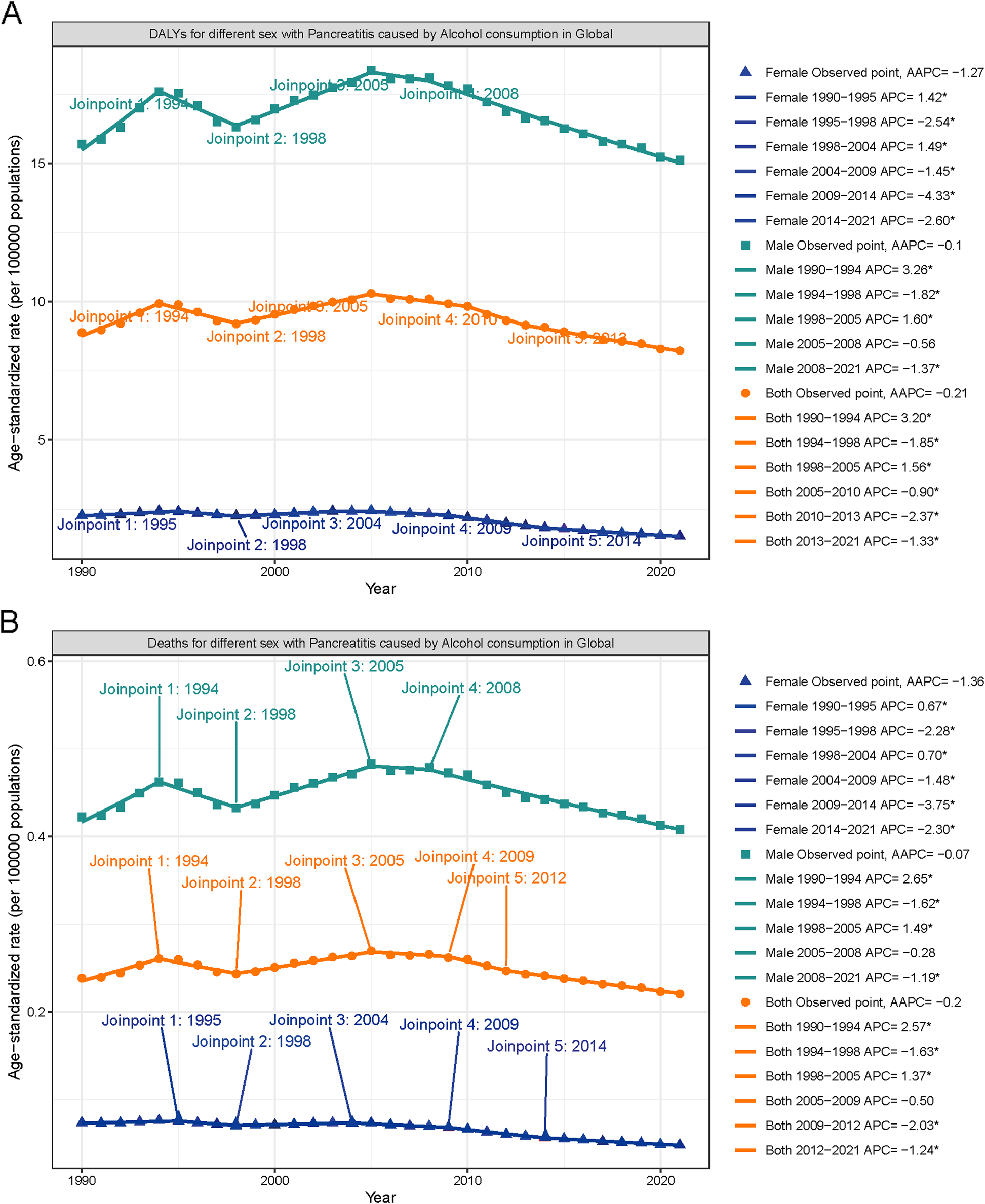
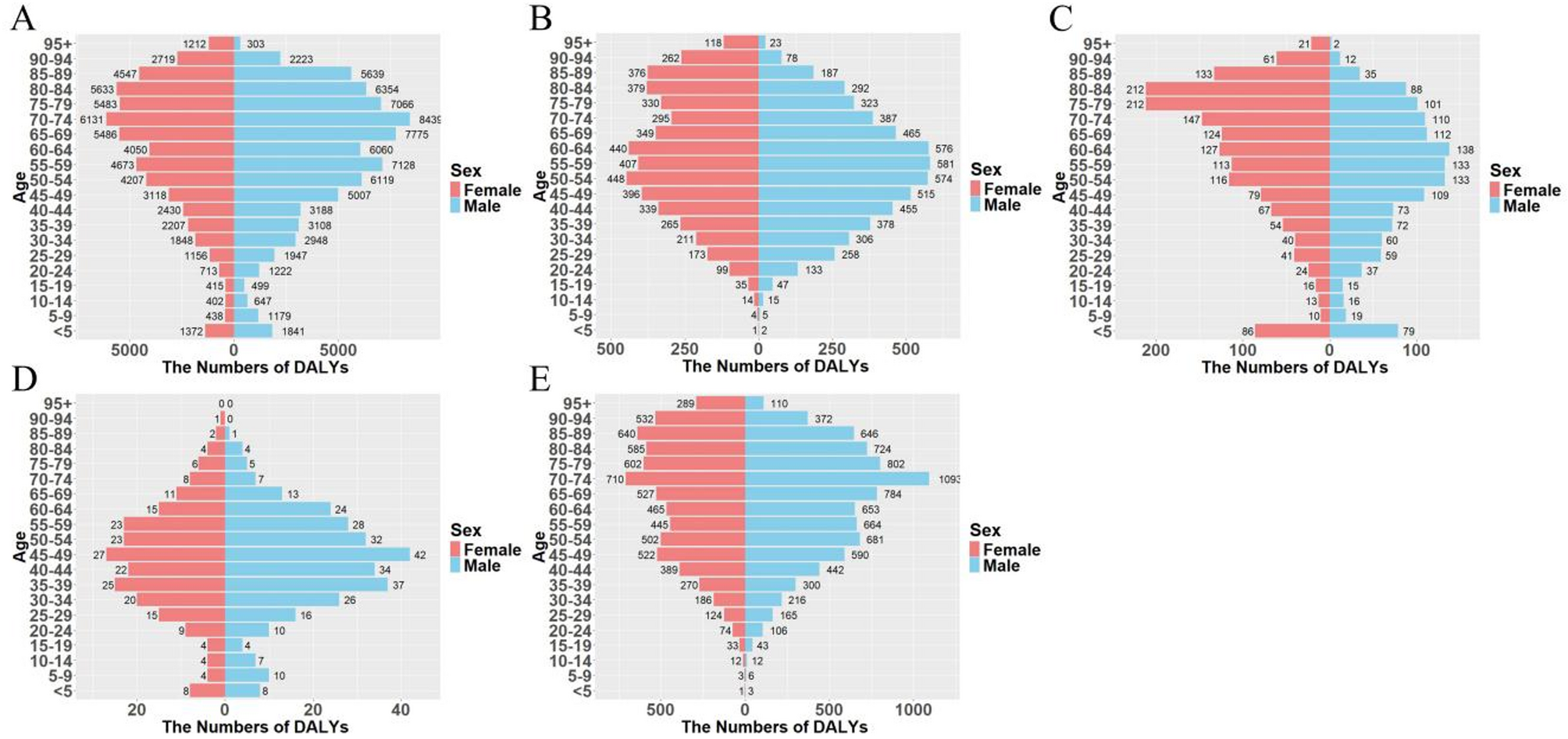
Global burden of acute pancreatitis attributable to high alcohol intake from 1990 to 2021: findings and prevention potential based on GBD 2021 | BMC Gastroenterology
Pancreatitis is an acute inflammatory disease caused by premature activation of pancreatic enzymes, leading to pancreatic injury and multiple organ dysfunction. Over the past three decades, its global prevalence has continued to rise [19, 21,
Continue Reading
-
The relationship between urine output and time to methotrexate clearance in pediatric leukemia patients receiving high-dose methotrexate therapy | BMC Cancer
As MTX continues to play a central role in the treatment of various malignancies, the balance between its therapeutic efficacy and potential toxicity must be carefully managed. Delayed MTX clearance is associated with an increased risk of AEs,…
Continue Reading
-
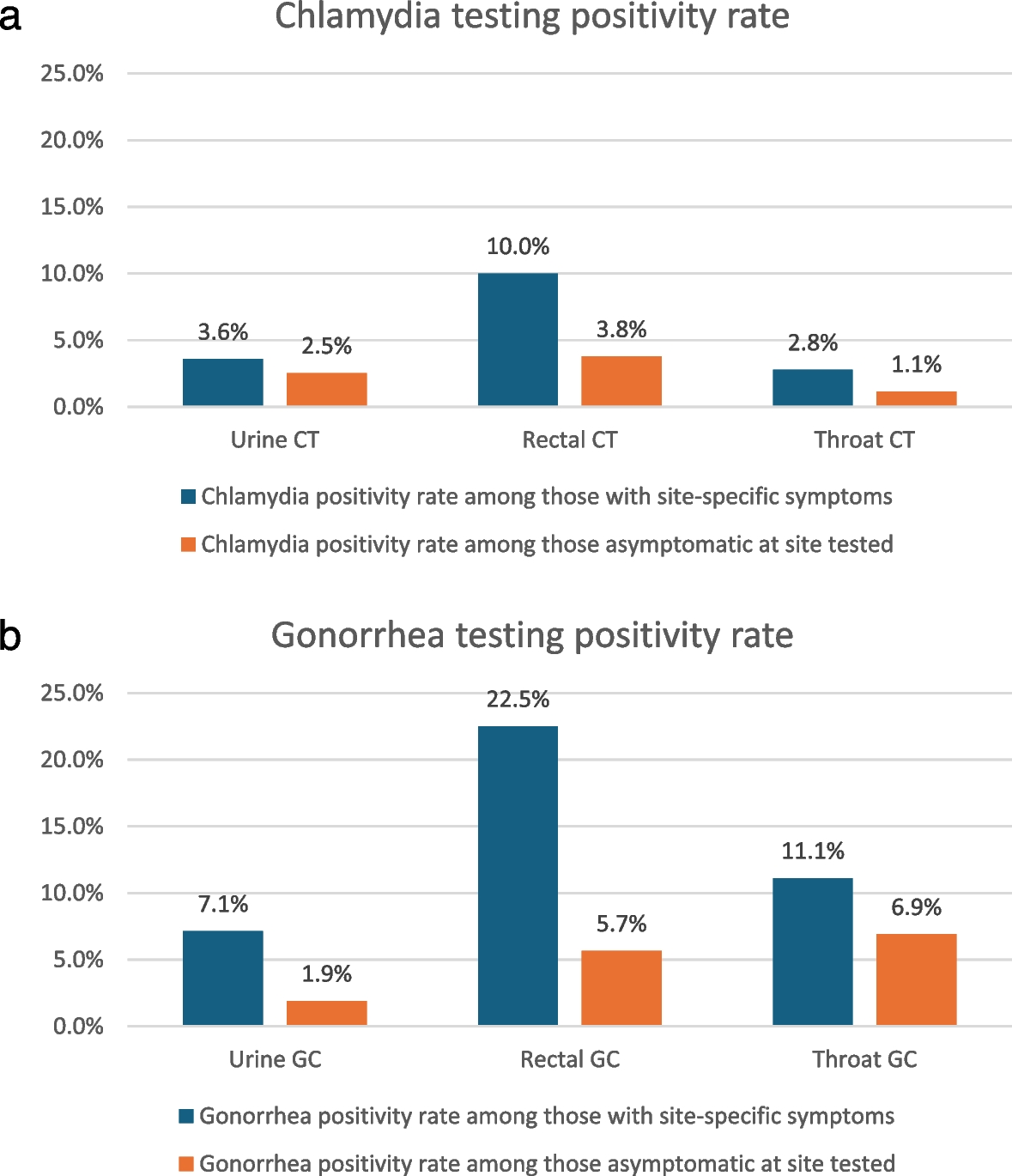
STI testing and diagnosis rates among patients with Mpox in 2 populous US cities, 2022 | BMC Medicine
Patient consent
This study was approved by the Columbia University Irving Medical Center Institutional Review Board, with a waiver of informed consent. This study was approved through the Committee for the Protection of Human Subjects at UTHealth,…
Continue Reading
-
The burden of inflammatory bowel disease in five East Asian countries an analysis based on the global burden of disease study 1990–2021 | BMC Gastroenterology
This study identified significant disparities in the burden of IBD across five East Asian countries, with a distinct correlation between these variations and each country’s socioeconomic development level (SDI) level. Through comparative…
Continue Reading
-
New JNCCN Study Confirms it’s ‘Never Too Late’ to See Survival Benefits from Quitting Smoking–Even With Late-Stage Cancer
Researchers found that patients with stage III or IV cancer who quit smoking gained nearly a full year of additional life over their counterparts who continued, highlighting the important role of smoking cessation support…
Continue Reading
-
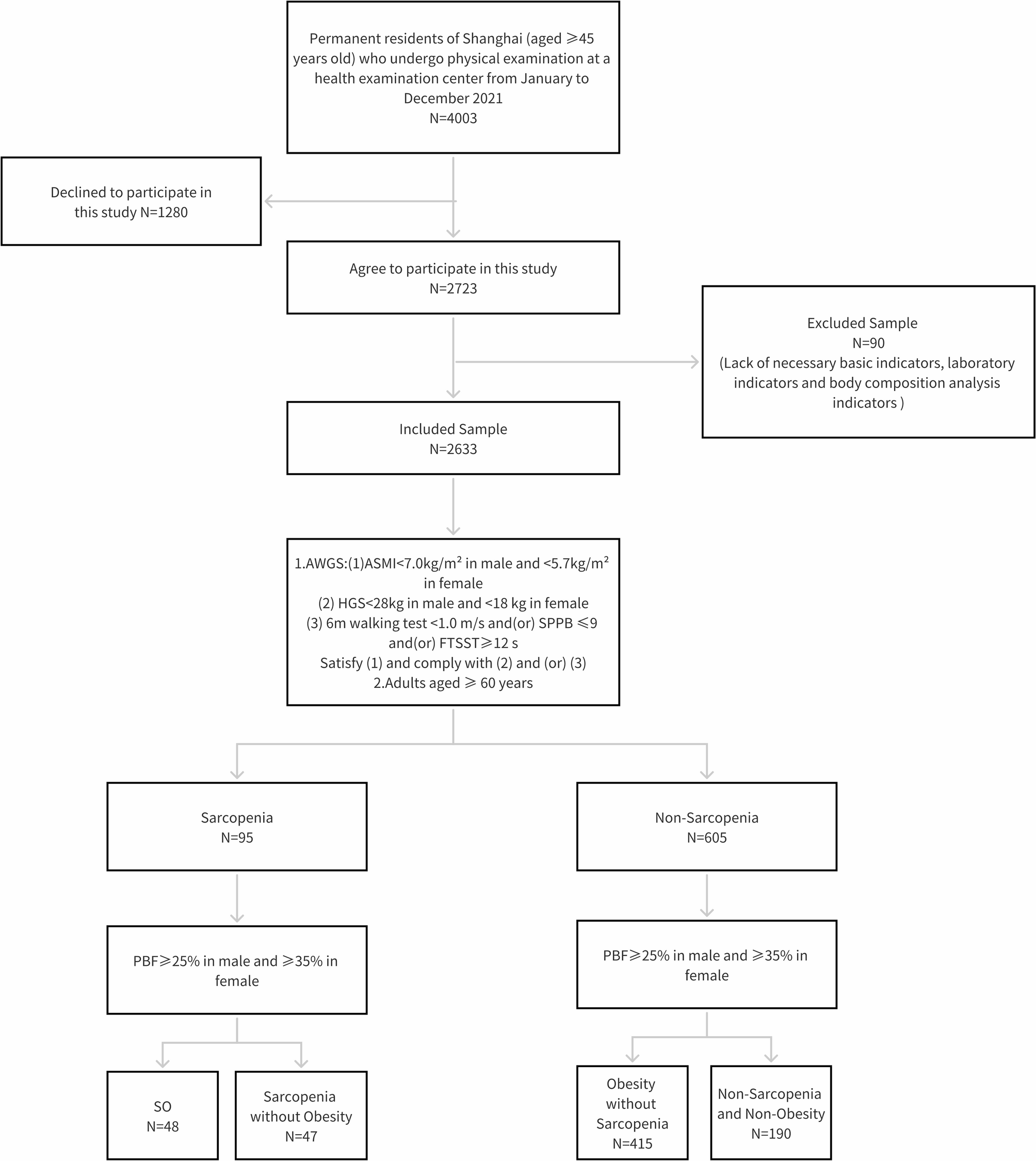
Study on body composition characteristics and influencing factors of sarcopenia status among older adults in Shanghai: a cross-sectional study | Journal of Health, Population and Nutrition
Study participants
Study design
Participants for this cross-sectional study were chosen among the attendees at a physical examination center in Shanghai using convenience sampling from July to December 2023. In order to protect patient privacy,…
Continue Reading
-
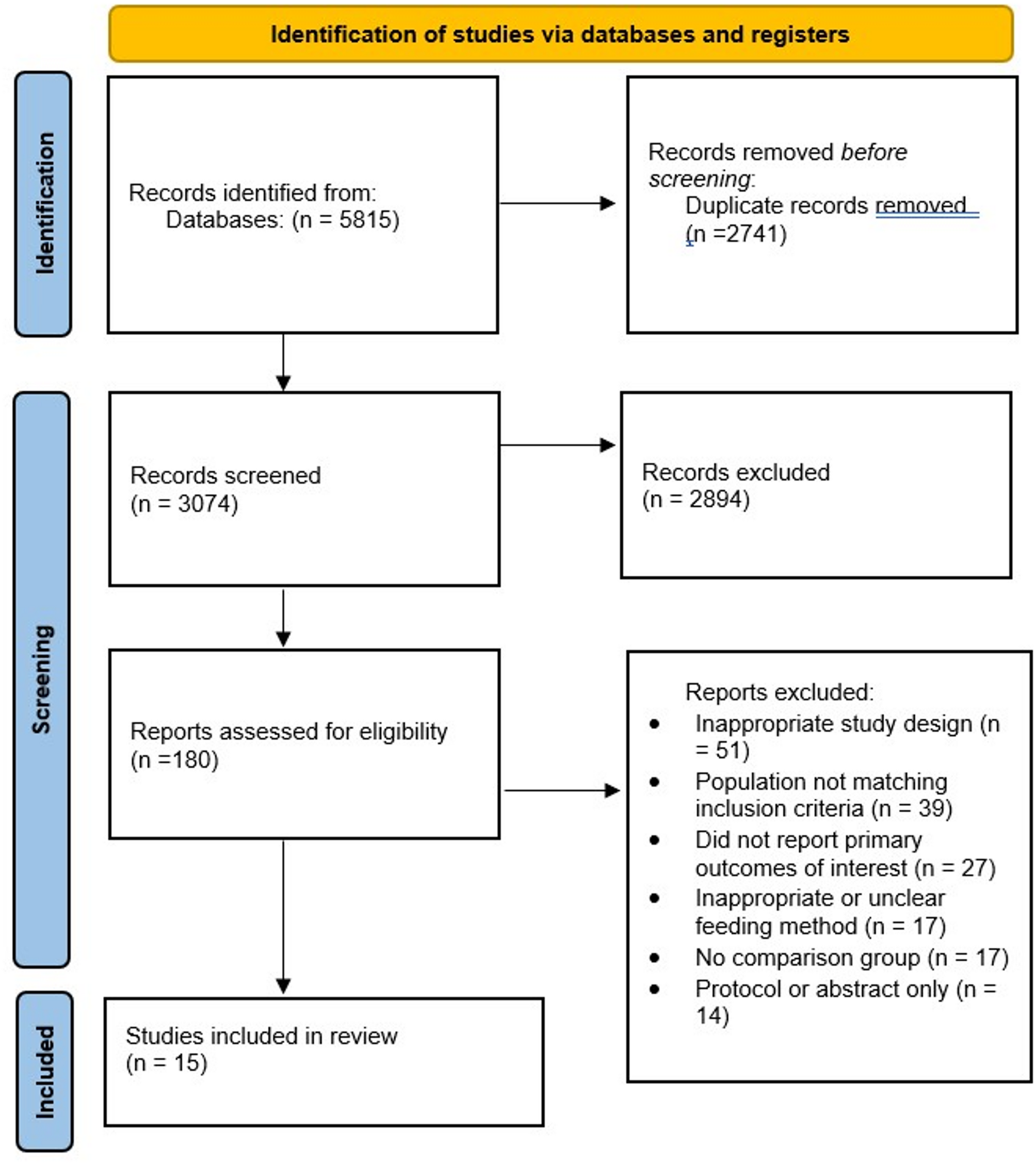
Early oral feeding after laparoscopic total gastrectomy in gastric cancer patients: a meta-analysis of randomized controlled trials and cohort studies | BMC Gastroenterology
Hospital stay duration
Fourteen studies [10, 19,20,21,22,23,24,25,26,27,28,29, 31, 32] were included to assess the effect of EOF versus TOF on the length of hospital stay (Fig. 2). A random-effects model showed a statistically significant…
Continue Reading