Many Americans choose food based on cost and nutrition, but personal values, such as animal welfare and environmental concerns, also shape what ends up on our plates.
Now, researchers at the Gerald J. and Dorothy R. Friedman…

Many Americans choose food based on cost and nutrition, but personal values, such as animal welfare and environmental concerns, also shape what ends up on our plates.
Now, researchers at the Gerald J. and Dorothy R. Friedman…

A recent analysis reveals that older adults with prior incarceration report worse physical and mental health than their peers, even if they were incarcerated in the distant past. The findings are published in the Journal of the…
Researchers from Osaka Metropolitan University have discovered how the balance of bacteria in the stomach affects the growth of neuroendocrine tumors (NETs). By identifying the specific bacteria involved and the biochemical…

Menopause before the age of 45 (known as early menopause) is associated with an increased risk of an array of serious diseases, including cardiovascular disease and osteoporosis. A new study suggests that it may also force women out…

Might brain damage linked to Alzheimer’s be one of the reasons dolphins lose their way and end up stranded? It’s a possibility explored in a new study of 20 common bottlenose dolphins (Tursiops truncatus) stranded in the Indian River Lagoon,…
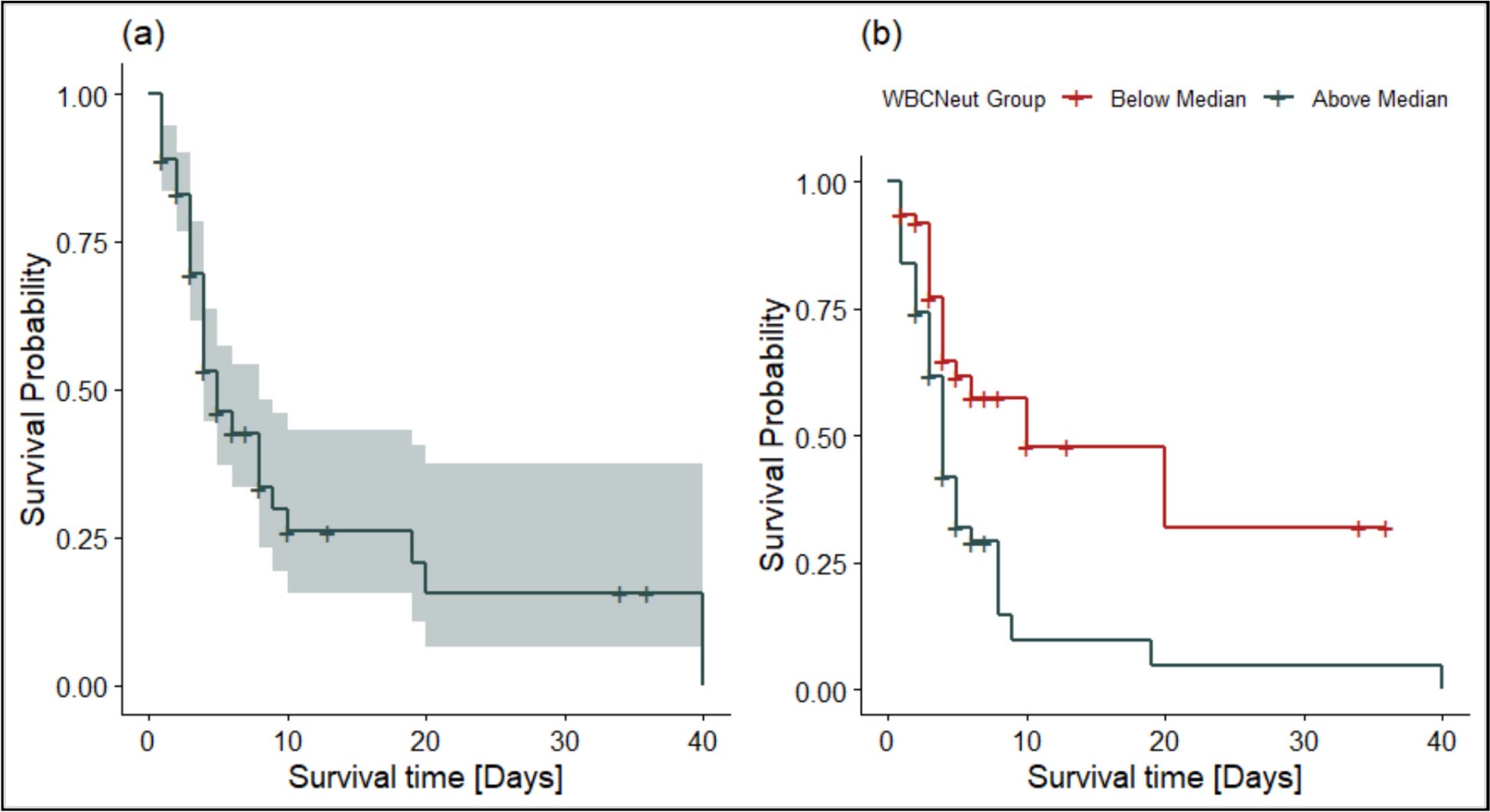
A total of 125 patients were followed up over 40 days. Of these, 56 (44.8%) were females and 67 (53.6%) were males. The proportion of deaths was marginally higher among males (56.7%) compared to females (50.0%), although this difference did not…
Current prostate specific antigen (PSA) testing “may not effectively target testing to those most likely to benefit, raising concerns about overtesting” warn researchers from the University of Oxford in a study of over 10 million…

A study published in JAMA Network Open identifies four distinct profiles of Nonverbal Learning Disability (NVLD), providing evidence that may help refine diagnostic criteria and guide more individualized approaches to care for…
Multiple sclerosis, or MS, is a chronic autoimmune disease affecting more than 2.9 million people worldwide. It occurs when the immune system mistakenly attacks the myelin sheath, the protective insulation around nerve fibers,…