Medicare beneficiaries with heart disease or major cardiovascular risk factors reported less cost-related medication non-adherence-skipping or reducing doses, delaying prescription fills or foregoing medications due to cost-after…
Category: 6. Health
-

Drug-releasing stitches aim to reduce inflammation and improve healing
Deep cuts from accidents or surgeries require stitches, typically followed by oral anti-inflammatory medications like ibuprofen. While these medications help with pain, they don’t act specifically on the wounds. Consequently, the…
Continue Reading
-
A New Clue Offers Hope Against The Deadliest Infection : ScienceAlert
After decades of decline in the developed world, tuberculosis (TB) is back on the rise, and increasingly resistant to our best antibiotics.
The World Health Organization (WHO) is calling it a public health crisis – but help may be on the…
Continue Reading
-
Covid-19 immunity likely to lower risk of another SARS pandemic – study
They found that as well as high levels of immunity to SARS-CoV-2, the virus responsible for the Covid-19 pandemic, the population also had immunity against a range of “sarbecoviruses” – the wider family of viruses to which SARS-CoV-2…
Continue Reading
-
Metabolite Sensors Improve Cancer Immunotherapy Results
A technique that transforms immune cells into cancer-seeking bloodhounds may overcome a roadblock that has hampered immunotherapy for solid tumors, according to a new study by Stanford Medicine researchers.
The approach equips certain types of…
Continue Reading
-
US vaccine demand at risk as childhood immunisation cuts threaten manufacturing – itij.com
- US vaccine demand at risk as childhood immunisation cuts threaten manufacturing itij.com
- What parents need to know about the CDC’s new child vaccine schedule Nebraska Medicine
- Confusion USA: universal childhood vaccines reduced The Medical…
Continue Reading
-
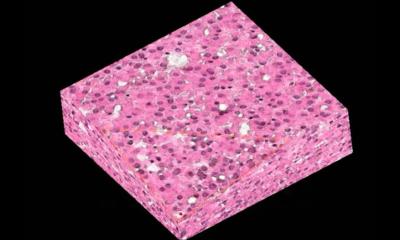
New X-ray technique could transform tissue diagnosis • healthcare-in-europe.com
The ability to visualise intact tissue in three dimensions, right down to structures as small and as important as a single cell, opens up so many possibilities in biomedical research and clinical practice
Michela Esposito
The device works by…
Continue Reading
-
World Tuberculosis Day: 1 out of 5 cases in Europe go undetected – Euronews.com
- World Tuberculosis Day: 1 out of 5 cases in Europe go undetected Euronews.com
- The European Region misses 1 in 5 TB cases: WHO Europe and ECDC publish new joint surveillance report Unric
- More than 1 in 5 new TB cases in Europe are missed, analysis…
Continue Reading
-
Study Challenges Long-Held Belief About Parkinson’s Tremors – SciTechDaily
- Study Challenges Long-Held Belief About Parkinson’s Tremors SciTechDaily
- Rest tremor in Parkinson’s linked to better-preserved dopamine function News-Medical
- Study Reveals Distinct Brain Mechanism Behind Parkinson’s Tremor The Indian…
Continue Reading
-
Long-Term Survivors of HIV Summit Takes Place This Week in Sitges
This week, from 25–28 March 2026, the European AIDS Treatment Group (EATG), together with Ribbon – A Center of Excellence (USA), The Reunion Project (USA), and Realize (Canada), is bringing together a powerful global community in Sitges,…
Continue Reading