
Researchers at WashU Medicine have developed a nasal vaccine against the highly pathogenic…
Category: 6. Health
-
One KP father’s story challenges polio myths
PESHAWAR: Every evening, as the sun dips behind the snow-dusted Koh-e-Sufaid mountains, 45-year-old Sajjad Ahmad wheels his younger daughter to the edge of a dusty playground in village…
Continue Reading
-
2 Nipah virus cases reported in India: WHO
(Xinhua) 13:08, January 31, 2026GENEVA, Jan. 30 (Xinhua) — The World Health Organization (WHO) said on Friday that two laboratory-confirmed cases of Nipah virus (NiV) infection have been reported in India.
In its latest Disease…
Continue Reading
-

Sporadic Nipah virus cases highlight importance of global surveillance
The Global Virus Network (GVN), representing eminent human and animal virologists from more than 90 Centers of Excellence and Affiliates in over 40 countries dedicated to advancing research, collaboration, and pandemic preparedness,…
Continue Reading
-
NA body informed: ‘Over 300,000 HIV cases reported in Pakistan’ – Business Recorder
- NA body informed: ‘Over 300,000 HIV cases reported in Pakistan’ Business Recorder
- No hospital licensed, illegal clinics flourish as Parliament exposes regulatory failure in Islamabad’s private healthcare sector Minute Mirror
- Pakistan on…
Continue Reading
-
2 Nipah virus cases reported in India: WHO-Xinhua
GENEVA, Jan. 30 (Xinhua) — The World Health Organization (WHO) said on Friday that two laboratory-confirmed cases of Nipah virus (NiV) infection have been reported in India.
In its latest Disease Outbreak News, the WHO said that the…
Continue Reading
-

Anxiety, depression linked to 78% higher risk of long COVID in older women
Older women with a history of anxiety and depressive symptoms were significantly more likely to develop long COVID than those without such symptoms, according to a large prospective analysis published this week in Menopause.
A University of…
Continue Reading
-

I Thought Lifting Heavy Weights Would Make Me Stronger—But It Ended Up Changing So Much More
I still remember the first time I walked into a weight room. I was completely, totally, and utterly overwhelmed by all the chunks of metal and clanking machines. I was a run-on -the-treadmill-and-duck-out-ASAP sort of person. A sometimes pilates…
Continue Reading
-
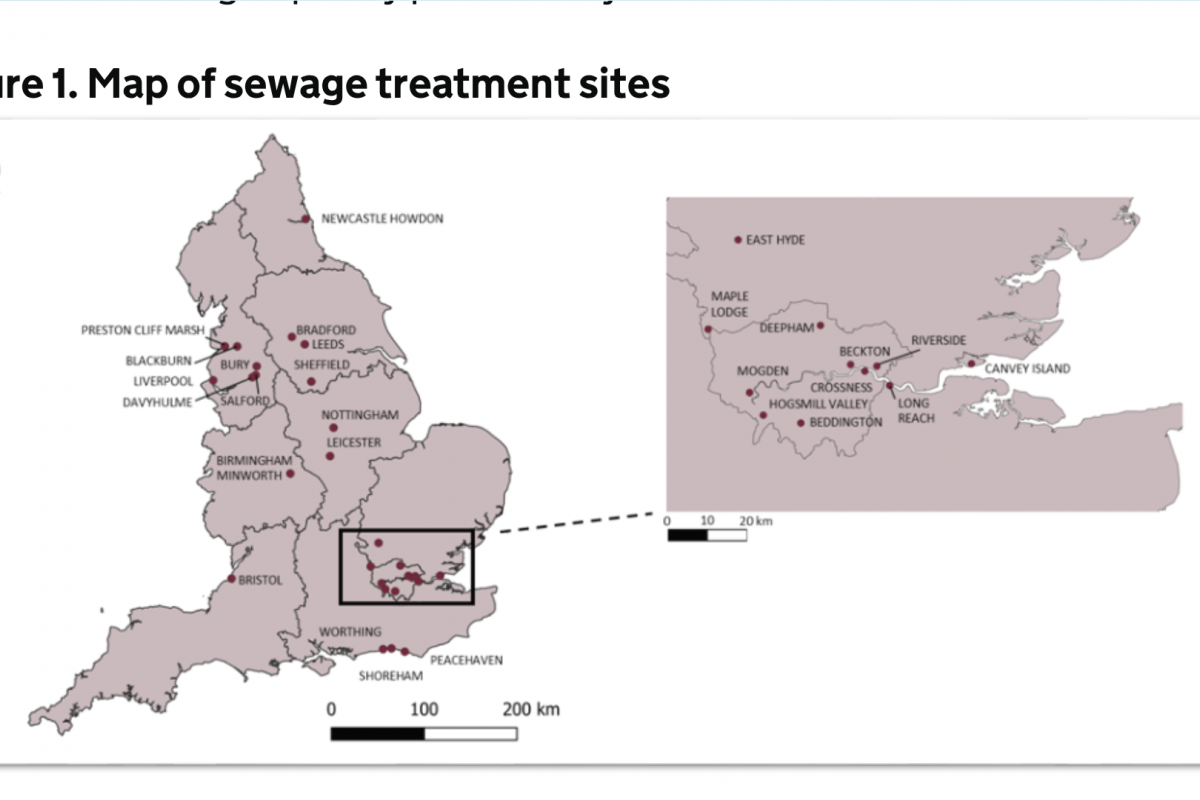
UK Confirms Poliovirus Detection in 2026 — Vax-Before-Travel
(Vax-Before-Travel News)Despite the United Kingdom (UK) maintaining high vaccination coverage and remaining polio-free for decades, recent detections of poliovirus in wastewater have emerged as a significant early warning signal.
As of January…
Continue Reading
-

GLP-1 drugs and alcohol reduction
Alcohol consumption continues its decline. The drinking rate in the US has reached a new low: today, the percentage of US adults who say they consume alcohol has fallen to 54%. People are becoming increasingly prioritizing health and wellness:…
Continue Reading